Neurocysticercosis (Taenia solium): Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
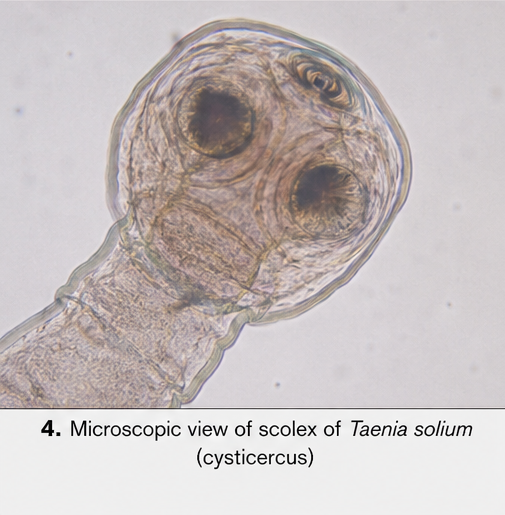
Neurocysticercosis is a parasitic infection of the central nervous system caused by the larval stage of Taenia solium. It is one of the leading causes of acquired epilepsy in developing countries and remains a significant public health concern. The clinical presentation is highly variable, depending on the number, size, location, and stage of the cysticerci within the brain.
We report the case of a 28-year-old male who presented with new-onset generalized tonic-clonic seizures and persistent headache. Neuroimaging revealed multiple cystic lesions with perilesional edema, consistent with neurocysticercosis. The patient was treated with antiparasitic therapy (Albendazole), corticosteroids, and antiepileptic drugs, resulting in clinical improvement and seizure control.
This case highlights the importance of early recognition, appropriate imaging, and a multidisciplinary management approach in improving outcomes in patients with neurocysticercosis.
Introduction
Neurocysticercosis is a central nervous system infection caused by ingestion of Taenia solium eggs, leading to the development of larval cysts (cysticerci) within neural tissue. Humans act as intermediate hosts following fecal-oral transmission, often through contaminated food or water.
The disease is endemic in regions with poor sanitation and inadequate hygiene practices. It is a major contributor to seizure disorders worldwide, particularly in low- and middle-income countries.
The clinical manifestations vary widely and may include seizures, headaches, focal neurological deficits, hydrocephalus, and cognitive disturbances. The disease progresses through different stages—vesicular, colloidal, granular nodular, and calcified—each with distinct radiological and clinical features.
Risk factors and associations include:
• Consumption of contaminated food or water
• Poor sanitation and hygiene
• Close contact with Taenia solium carriers
• Residence in endemic areas
• Lack of proper meat inspection
Early diagnosis and appropriate treatment are essential to reduce morbidity and prevent long-term neurological complications.
Case Report
Patient History
A 28-year-old male presented to the emergency department with:
• Two episodes of generalized tonic-clonic seizures within 24 hours
• Persistent headache for the past 2 weeks
• Occasional nausea without vomiting
• No history of fever, trauma, or prior seizures
The seizures were sudden in onset, lasted approximately 1–2 minutes, and were followed by postictal confusion.
The patient reported a history of consuming undercooked pork occasionally and lived in a rural area with limited sanitation facilities.
There was no significant past medical history, and no family history of epilepsy or neurological disorders.
Clinical Examination
General Examination
• Patient was conscious but drowsy postictally
• Vital signs were stable
• No signs of systemic infection
Neurological Examination
• No focal motor deficits
• Cranial nerves intact
• Normal sensory examination
• Mild neck stiffness absent
• Fundoscopy: No papilledema
Systemic Examination
• Cardiovascular, respiratory, and abdominal examinations were unremarkable
Clinical Evaluation
Differential Diagnosis
Based on clinical presentation, the following conditions were considered:
• Neurocysticercosis
• Tuberculoma
• Brain metastasis
• Pyogenic brain abscess
• Primary seizure disorder
The acute onset of seizures with headache and epidemiological background raised suspicion for a parasitic or infectious etiology.
Investigations
Neuroimaging
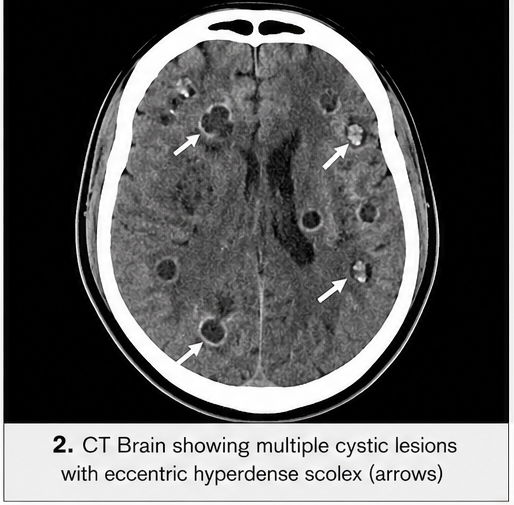
CT Scan of the Brain
• Multiple small cystic lesions in the cerebral cortex
• Some lesions showed eccentric hyperdense nodules (scolex)
• Surrounding perilesional edema
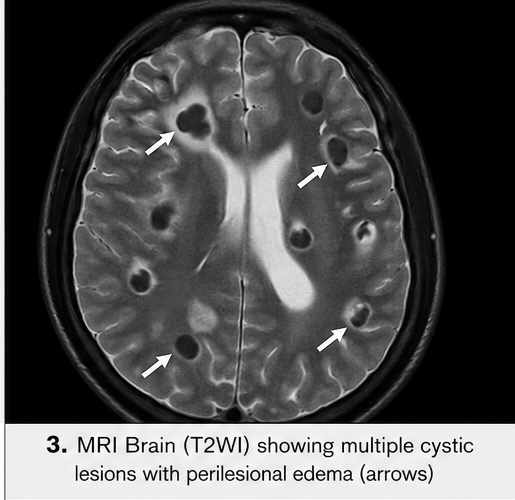
MRI Brain
• Multiple ring-enhancing lesions in the parietal and frontal lobes
• Lesions in different stages (vesicular and colloidal)
• Perilesional edema with mild mass effect
These findings were highly suggestive of neurocysticercosis.
Laboratory Investigations
• Complete blood count: Mild eosinophilia
• ESR: Mildly elevated
• Liver and renal function tests: Within normal limits
Serological Tests
• Enzyme-linked immunoelectrotransfer blot (EITB): Positive for Taenia solium antibodies
CSF Analysis (not performed due to absence of signs of raised intracranial pressure)
Diagnosis
Based on clinical presentation, imaging findings, and serological confirmation, a diagnosis of parenchymal neurocysticercosis with active lesions was established.
Management and Outcome
Management Strategy
The treatment plan was guided by:
• Number and location of lesions
• Stage of cysts
• Presence of edema
• Severity of symptoms
Medical Management
Antiepileptic Therapy
• Initiated with levetiracetam for seizure control
Antiparasitic Therapy
• Albendazole (15 mg/kg/day) administered for 14 days
Corticosteroids
• Prednisolone started prior to antiparasitic therapy to reduce inflammatory response
• Gradually tapered over 2 weeks
Supportive Care
• Analgesics for headache
• Antiemetics as needed
Clinical Course
During hospitalization:
• No further seizures were observed
• Headache improved significantly
• No signs of increased intracranial pressure
Follow-Up
At 1-Month Follow-Up:
• Patient remained seizure-free
• Mild residual headache
• Good compliance with medications
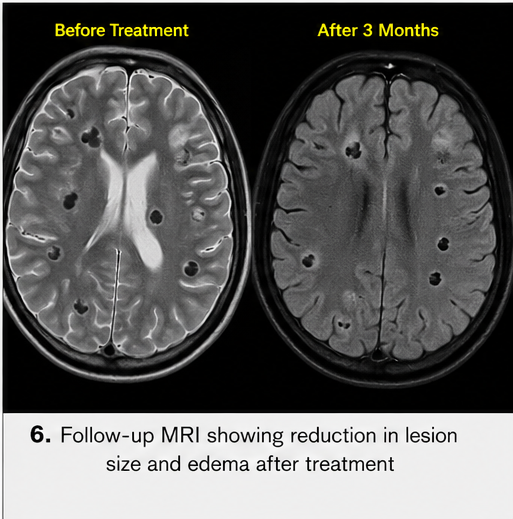
At 3-Month Follow-Up:
• Repeat MRI showed reduction in lesion size
• Decreased perilesional edema
• Some lesions progressed to calcified stage
At 6-Month Follow-Up:
• No recurrence of seizures
• Antiepileptic therapy continued
• Patient resumed normal daily activities
Overall, the patient demonstrated favorable clinical and radiological outcomes.
Discussion
Pathophysiology
Neurocysticercosis results from ingestion of Taenia solium eggs, which hatch in the intestine and release oncospheres. These penetrate the intestinal wall and disseminate hematogenously to the central nervous system, where they develop into cysticerci.
The disease evolves through four stages:
• Vesicular stage – viable cysts with minimal inflammation
• Colloidal stage – cyst degeneration with intense inflammatory response
• Granular nodular stage – further degeneration and fibrosis
• Calcified stage – inactive lesions with residual calcifications
Clinical symptoms are primarily due to host inflammatory response rather than the parasite itself.
Epidemiology
• Common in Latin America, Africa, and Asia
• Leading cause of acquired epilepsy worldwide
• Higher prevalence in rural and low-resource settings
Clinical Manifestations
• Seizures (most common presentation)
• Chronic headaches
• Focal neurological deficits
• Raised intracranial pressure
• Hydrocephalus (in ventricular involvement)
Diagnostic Considerations
Diagnosis is based on a combination of:
• Clinical features
• Neuroimaging (CT/MRI)
• Serological tests
Characteristic imaging findings include:
• Cystic lesions with scolex
• Ring enhancement
• Calcifications
MRI is more sensitive for detecting viable cysts and ventricular involvement.
Treatment Considerations
Management depends on lesion type and symptom severity.
Antiparasitic Therapy:
• Albendazole (preferred)
• Praziquantel (alternative)
Anti-inflammatory Therapy:
• Corticosteroids to reduce edema and inflammation
Seizure Management:
• Long-term antiepileptic drugs
Surgical Intervention:
• Reserved for hydrocephalus or large cysts
• Ventriculoperitoneal shunting in selected cases
Complications
Potential complications include:
• Recurrent seizures
• Chronic epilepsy
• Hydrocephalus
• Increased intracranial pressure
• Cognitive impairment
Treatment-related complications:
• Inflammatory worsening after antiparasitic therapy
• Steroid-related adverse effects
Prognosis
The prognosis of neurocysticercosis is generally favorable with timely treatment.
Factors influencing outcomes:
• Number and location of lesions
• Stage of disease
• Treatment adherence
• Presence of complications
Calcified lesions may persist and remain a focus for future seizures.
Conclusion
Neurocysticercosis is a significant cause of neurological morbidity, particularly in endemic regions. It commonly presents with seizures and requires a high index of suspicion for diagnosis.
This case emphasizes the importance of integrating clinical history, epidemiological factors, and neuroimaging findings for accurate diagnosis. Early initiation of antiparasitic therapy, corticosteroids, and antiepileptic drugs plays a crucial role in improving patient outcomes.
Preventive strategies, including improved sanitation, health education, and proper food handling, are essential in reducing disease burden.
Timely diagnosis, individualized management, and regular follow-up are key to achieving optimal clinical outcomes and preventing long-term neurological sequelae.
References
- White, A. C. (2000). Neurocysticercosis: Updates on epidemiology, pathogenesis, diagnosis, and management. Annual Review of Medicine. https://pubmed.ncbi.nlm.nih.gov/10671284/
- Del Brutto, O. H., et al. (2017). Revised diagnostic criteria for neurocysticercosis. Journal of the Neurological Sciences. https://pubmed.ncbi.nlm.nih.gov/28457777/
- García, H. H., et al. (2002). Clinical symptoms, diagnosis, and treatment of neurocysticercosis. Lancet Neurology. https://pubmed.ncbi.nlm.nih.gov/12849240/
- Nash, T. E., & Garcia, H. H. (2011). Diagnosis and treatment of neurocysticercosis. Nature Reviews Neurology. https://pubmed.ncbi.nlm.nih.gov/21304416/
- Carpio, A., et al. (2016). New diagnostic criteria for neurocysticercosis: Reliability and validity. Annals of Neurology. https://pubmed.ncbi.nlm.nih.gov/26813787/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge