Nipah Virus Encephalitis: Clinical Presentation, Diagnostic Challenges, Infection Control Measures, and Multidisciplinary Management — A Case Report
OthersPage Navigation
Abstract
Nipah virus (NiV) is a highly pathogenic zoonotic virus associated with sporadic outbreaks of severe encephalitis and respiratory illness, predominantly in South and Southeast Asia. The infection carries a high case fatality rate and poses significant public health concerns due to its potential for human-to-human transmission and lack of specific antiviral therapy. Clinical presentation is often nonspecific in the early phase, which may delay diagnosis and increase the risk of secondary transmission.
We report a confirmed case of Nipah virus encephalitis in a young adult presenting with acute febrile illness and rapidly progressive neurological deterioration during a regional outbreak. This case highlights the importance of early epidemiological suspicion, timely laboratory confirmation, strict infection prevention protocols, and coordinated multidisciplinary care. The report also discusses diagnostic challenges, radiological features, management strategies, and follow-up outcomes in the context of existing literature.
Introduction
Nipah virus is an emerging zoonotic paramyxovirus belonging to the genus Henipavirus within the family Paramyxoviridae. Since its first identification during an outbreak among pig farmers in Malaysia in 1998–1999, Nipah virus has been recognized as a cause of recurrent outbreaks with high mortality in countries such as Bangladesh and India [1]. Fruit bats of the genus Pteropus serve as the natural reservoir, with spillover to humans occurring via consumption of contaminated food products, contact with infected animals, or direct human-to-human transmission [2].
The clinical spectrum of Nipah virus infection ranges from asymptomatic disease to acute febrile illness, severe encephalitis, and acute respiratory distress syndrome. Neurological involvement is the predominant and most life-threatening manifestation, often progressing rapidly to coma and death [3]. The absence of approved antiviral therapy and vaccines for human use underscores the importance of early diagnosis, supportive care, and rigorous infection control measures.
This case report describes a laboratory-confirmed case of Nipah virus encephalitis, emphasizing clinical features, diagnostic workup, radiological findings, therapeutic challenges, and multidisciplinary management in an outbreak setting.
Case Report
Patient History
A 26-year-old male agricultural worker presented to the emergency department with a four-day history of high-grade fever, severe headache, and generalized body aches. This was followed by vomiting and progressive alteration in sensorium over the preceding 24 hours. The patient was previously healthy, with no known chronic medical conditions.
The patient had recently returned from a rural district reporting confirmed cases of Nipah virus infection. He admitted to frequent consumption of locally harvested fruits and raw date palm sap. There was no history of animal bites, but possible exposure to bat-contaminated environments could not be excluded. No similar illness was reported among immediate family members at presentation.
Clinical Examination
On admission, the patient appeared acutely ill and disoriented. Vital signs revealed a temperature of 39.3°C, pulse rate of 112 beats per minute, blood pressure of 100/60 mmHg, and respiratory rate of 22 breaths per minute. Oxygen saturation was 94% on room air.
Neurological examination showed altered mental status with a Glasgow Coma Scale score of 11/15. The patient was confused and responded inappropriately to verbal commands. Neck stiffness was present. No focal motor deficits were noted initially. Pupillary reflexes were normal. There were no skin rashes, petechiae, or lymphadenopathy.
Respiratory examination revealed bilateral basal crepitations. Cardiovascular and abdominal examinations were unremarkable, with no hepatosplenomegaly detected.
Clinical Evaluation
Initial Differential Diagnosis
Based on clinical presentation and epidemiological exposure, the following differential diagnoses were considered:
• Viral encephalitis (including Nipah virus)
• Acute bacterial meningoencephalitis
• Cerebral malaria
• Autoimmune encephalitis
• Metabolic or toxic encephalopathy
Given the ongoing regional outbreak and neurological involvement, Nipah virus infection was prioritized as a probable diagnosis.
Investigations
Laboratory Studies
Initial laboratory investigations showed:
• Hemoglobin: 13.2 g/dL
• Total leukocyte count: 15,600/µL (neutrophil predominance)
• Platelet count: 118,000/µL
• Serum electrolytes: Mild hyponatremia
• Liver enzymes: Mild elevation of transaminases
• Renal function tests: Within normal limits
Cerebrospinal fluid (CSF) analysis revealed lymphocytic pleocytosis with elevated protein levels and normal glucose, consistent with viral encephalitis. Blood cultures were sterile, and peripheral smear was negative for malarial parasites.
Radiological Evaluation
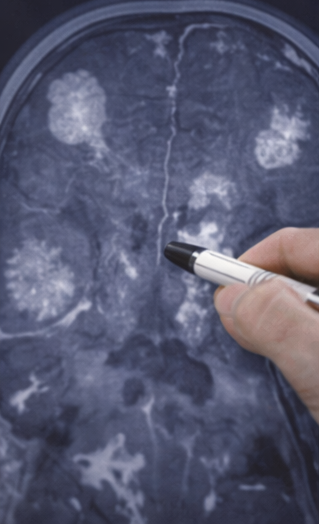
Magnetic resonance imaging (MRI) of the brain demonstrated multiple discrete hyperintense lesions in the subcortical white matter, basal ganglia, and brainstem on T2-weighted and FLAIR sequences. These findings were suggestive of viral encephalitis.
Chest radiography revealed bilateral patchy opacities, raising suspicion of early pulmonary involvement. No pleural effusion was noted.
Diagnosis
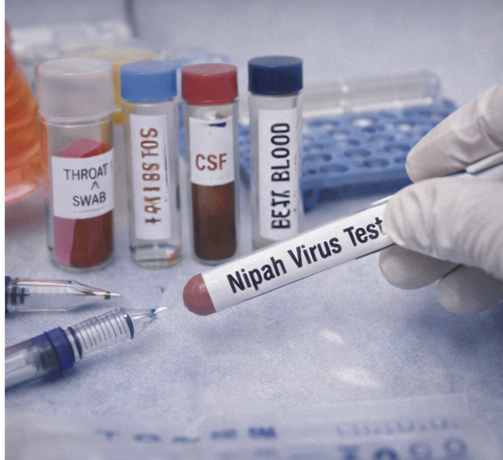
Throat swab, blood, and CSF samples were sent to a reference laboratory for Nipah virus testing under biosafety level-4 protocols. Reverse transcription–polymerase chain reaction (RT-PCR) returned positive for Nipah virus RNA. Serological testing showed the presence of Nipah virus–specific IgM antibodies.
The diagnosis of Nipah virus encephalitis was confirmed based on clinical features, epidemiological exposure, neuroimaging findings, and laboratory confirmation.
Management and Outcome
Multidisciplinary Approach
The patient was transferred to a designated isolation intensive care unit.

Management involved a multidisciplinary team including infectious disease specialists, neurologists, intensivists, microbiologists, nursing staff trained in infection control, and public health officials.

Strict barrier nursing and personal protective equipment protocols were enforced.
Contact tracing was initiated for healthcare workers and family members, and local health authorities were notified as per national surveillance guidelines.
Therapeutic Management
Treatment was primarily supportive. The patient received intravenous fluids, antipyretics, and electrolyte correction. Empirical broad-spectrum antibiotics and antivirals were initially administered and later de-escalated once bacterial causes were excluded.
Due to worsening sensorium and development of generalized tonic-clonic seizures, anticonvulsants were initiated. Mechanical ventilation was required following respiratory deterioration. Ribavirin was administered on a compassionate-use basis, although its efficacy remains inconclusive.
Follow-Up and Outcome
After ten days of intensive care support, the patient showed gradual neurological improvement. He was successfully weaned off mechanical ventilation and transferred to a step-down unit. Cognitive deficits, including memory impairment and slowed processing, were noted during recovery.
At discharge after four weeks, the patient was ambulatory with mild residual cognitive dysfunction and was referred for neurorehabilitation. At three-month follow-up, significant improvement was observed, with the patient regaining near-normal functional status.
Discussion
Nipah virus encephalitis remains a critical public health threat due to its high mortality, potential for outbreaks, and absence of targeted therapy. Neurological manifestations dominate the clinical course, and respiratory involvement further worsens prognosis [4].
Early clinical recognition is challenging due to nonspecific initial symptoms. However, epidemiological history plays a crucial role in raising suspicion. Neuroimaging findings of multifocal white matter lesions are characteristic but not pathognomonic. Laboratory confirmation through RT-PCR remains the diagnostic gold standard [5].
This case underscores the importance of multidisciplinary management and strict infection control measures to reduce mortality and prevent secondary transmission. Long-term neurological sequelae are common among survivors, emphasizing the need for structured follow-up and rehabilitation.
Conclusion
Nipah virus infection should be considered in patients presenting with acute febrile encephalitis in endemic or outbreak-prone regions. Prompt diagnosis, aggressive supportive care, rigorous infection control practices, and coordinated multidisciplinary management are essential for improving patient outcomes and limiting transmission. Continued surveillance, research into antiviral therapies, and vaccine development are critical to addressing the ongoing threat posed by Nipah virus.
References
- Chua KB. Nipah virus outbreak in Malaysia. J Clin Virol. 2003;26(3):265–275.
- Luby SP. The pandemic potential of Nipah virus. Antiviral Res. 2013;100(1):38–43.
- Arunkumar G, et al. Outbreak investigation of Nipah virus disease in India. N Engl J Med. 2019;380:1258–1267.
- Ang BSP, Lim TCC, Wang L. Nipah virus infection. J Clin Microbiol. 2018;56(6):e01875-17.
- WHO. Nipah virus fact sheet. World Health Organization; 2023.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Breast Cancer Patients Living Longer Post-Medicaid Expansion
2.
Error on the MGUS-Autoimmune Disease Association.
3.
Patients with chronic myeloid leukemia who take nilotinib are at higher risk for diabetes and hyperlipidemia.
4.
The majority of cancer medications that receive expedited approval end up failing confirmatory trials.
5.
Unified Neuro/Psych Residency Program: New Proposal.
1.
Optimizing Melanoma Treatment: Strategies in Diagnosis, Clinical Research, and Physician Training
2.
Hemoglobin C: Understanding its Role in Sickle Cell Disease
3.
Beyond the Human Eye: How AI Is Redefining Brain Cancer Diagnosis Through Advanced Imaging
4.
Understanding Abemaciclib: A Breakthrough Treatment for Breast Cancer
5.
The Growing Challenge of Haematological Malignancies in Older Adults
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Revolutionizing Treatment of ALK Rearranged NSCLC with Lorlatinib - Part II
2.
Exploring Potentials of Lorlatinib: The Third Generation ALK-TKI Through CROWN Trial
3.
Molecular Contrast: EGFR Axon 19 vs. Exon 21 Mutations - Part VII
4.
A Conclusive Discussion on CROWN Trial and the Dawn of a New Era in Frontline Management of ALK+ NSCLC
5.
Efficient Management of First line ALK-rearranged NSCLC - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge