HPV-Related Genital Warts: Clinical Presentation, Diagnosis, and Management- A Case Report
OthersPage Navigation
Abstract
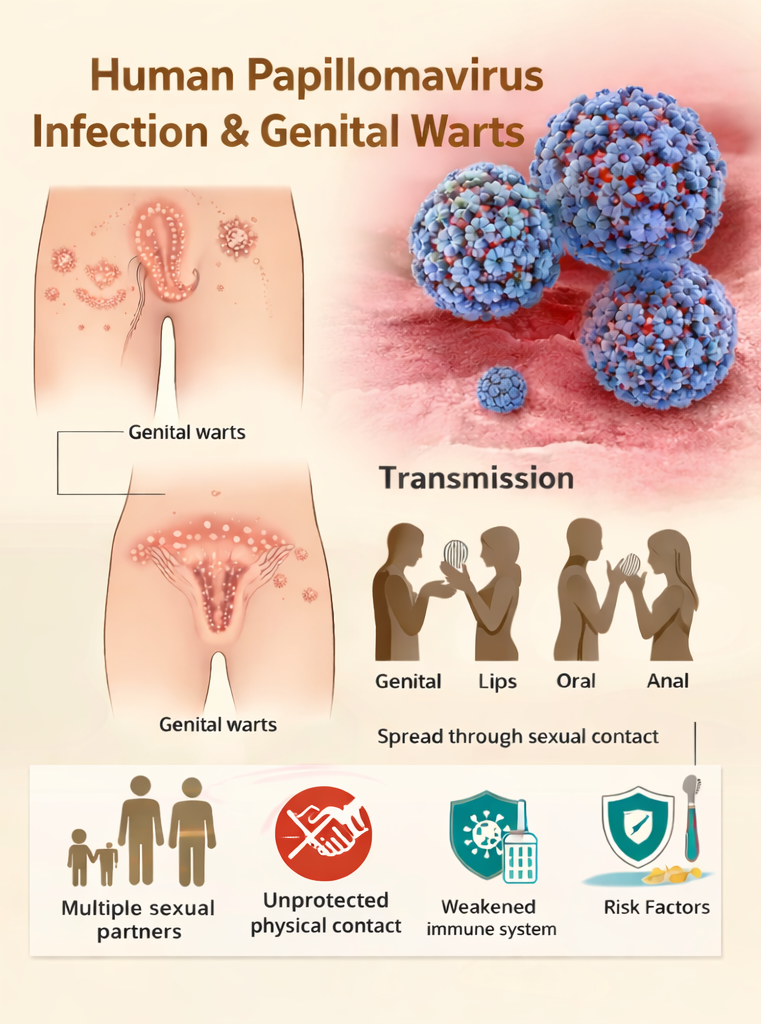
Genital warts (condyloma acuminata) are a common sexually transmitted infection caused primarily by low-risk human papillomavirus (HPV) types 6 and 11. They present as exophytic, flesh-colored or hyperpigmented papules and plaques on the anogenital skin and mucosa. Although benign, genital warts are associated with significant psychological distress, stigma, and high recurrence rates. Diagnosis is usually clinical but may be challenging due to variable morphology and overlap with other anogenital dermatoses. We report a confirmed case of genital warts in a young adult male presenting with multiple asymptomatic verrucous lesions over the penile shaft and perianal region. This case highlights the clinical presentation, diagnostic challenges, confirmatory evaluation, treatment approach, counseling regarding sexual health, and clinical outcome. The report emphasizes the importance of early recognition, patient education on transmission and recurrence, partner notification, and adherence to therapy for sustained clearance.
Introduction
Genital warts are among the most prevalent sexually transmitted infections worldwide and are caused predominantly by non-oncogenic HPV types 6 and 11. HPV is a DNA virus with tropism for squamous epithelium and is transmitted primarily through sexual contact. Most infections are asymptomatic and self-limiting; however, persistent infection may lead to clinically apparent warts.
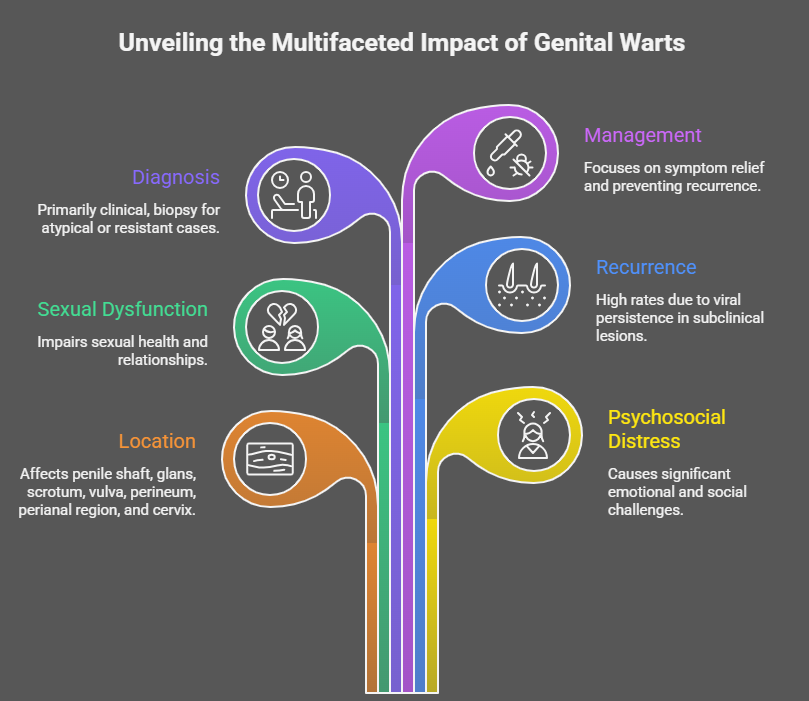
Genital warts commonly affect the penile shaft, glans, scrotum, vulva, perineum, perianal region, and cervix. Although medically benign, the disease is associated with psychosocial distress, sexual dysfunction, and high recurrence rates due to viral persistence in subclinical lesions. Diagnosis is primarily clinical, and biopsy is reserved for atypical or treatment-resistant lesions. This case report illustrates the clinical features, diagnostic considerations, management strategy, and outcome of a patient with genital warts due to HPV infection.
Case Report
Patient History
A 24-year-old man presented to the sexually transmitted infections (STI) clinic with a 2-month history of multiple painless growths over the penile shaft and perianal region. The lesions had gradually increased in number and size. The patient reported occasional itching but no bleeding, discharge, dysuria, or systemic symptoms.
He reported unprotected sexual contact with multiple partners over the past year. There was no prior history of similar lesions, sexually transmitted infections, or immunosuppressive conditions. He denied HIV infection and was not on long-term medications. The patient had not received HPV vaccination.
Clinical Examination
Examination revealed multiple soft, flesh-colored to hyperpigmented, verrucous papules and plaques over the penile shaft and perianal skin, some of which had coalesced into cauliflower-like lesions. The lesions were non-tender and non-ulcerated. No inguinal lymphadenopathy was present. The oral cavity and other mucocutaneous sites were normal.

Clinical Evaluation
Differential Diagnosis
The differential diagnoses included:
• Condyloma acuminata (genital warts)
• Condyloma lata (secondary syphilis)
• Molluscum contagiosum
• Seborrheic keratosis
• Bowenoid papulosis
The verrucous morphology, distribution, absence of systemic symptoms, and sexual history favored genital warts.
Investigations
Diagnosis was made clinically.
Screening for sexually transmitted infections, including HIV, syphilis (VDRL), hepatitis B, and hepatitis C, was advised as per standard STI protocols. All tests were negative.
Biopsy was not required as the lesions were typical in appearance and there were no features suggestive of malignancy such as ulceration, bleeding, pigmentation change, or induration.
Diagnosis
Based on clinical findings and risk factors, a diagnosis of genital warts (condyloma acuminata) secondary to HPV infection was established.
Management and Outcome
Management Strategy
The patient was treated with topical imiquimod 5% cream applied three times per week at night for up to 16 weeks.

Cryotherapy was offered as an alternative option, but the patient preferred topical therapy.
Comprehensive counseling was provided regarding:
• The viral etiology and sexually transmitted nature of the disease
• The possibility of recurrence despite treatment
• The importance of condom use to reduce transmission risk
• Partner notification and evaluation
• HPV vaccination for future protection
He was advised to abstain from sexual contact until visible lesions resolved.
Follow-Up and Outcome
At 6-week follow-up, a significant reduction in lesion size and number was observed, with mild local erythema reported as a side effect of imiquimod. At 12 weeks, near-complete clearance of lesions was achieved.
At 6-month follow-up, no new lesions were noted. The patient received HPV vaccination and reported consistent condom use. He was advised to return for early evaluation if any recurrence occurred.
Discussion
Genital warts represent a common manifestation of low-risk HPV infection, predominantly affecting sexually active young adults. The disease burden is substantial due to high transmission rates, recurrence, and psychosocial impact. Clinical diagnosis is usually sufficient; however, atypical lesions require biopsy to exclude premalignant or malignant conditions.
Treatment options include patient-applied therapies (imiquimod, podophyllotoxin) and provider-administered therapies (cryotherapy, trichloroacetic acid, electrocautery). No therapy eradicates HPV from the body; therefore, recurrence is common. HPV vaccination significantly reduces the risk of infection with vaccine-covered HPV types and should be strongly recommended.
Conclusion
Genital warts due to HPV infection are a common, benign, yet psychologically distressing condition with a high potential for recurrence owing to viral persistence in clinically inapparent tissue. Although the lesions are non-malignant in most cases, their chronicity, stigma, and impact on sexual health and self-esteem contribute to a substantial psychosocial burden for affected individuals. This case underscores the importance of timely clinical recognition, accurate diagnosis, and appropriate selection of patient-applied or provider-administered therapies based on disease extent, lesion morphology, and patient preference.
In addition, comprehensive STI screening, partner notification, and structured patient education regarding transmission dynamics, recurrence risk, and safe sexual practices are essential components of management. Preventive strategies, particularly HPV vaccination, play a critical role in reducing the incidence of new infections and recurrent disease at the population level. Early intervention, adherence to treatment, and longitudinal follow-up, combined with counseling and vaccination, can significantly improve clinical outcomes, limit onward transmission, and enhance overall patient well-being and quality of life.
References
- Lacey CJN, Lowndes CM, Shah KV. Burden and management of human papillomavirus-related disease. Vaccine. 2006;24(Suppl 3):S3/35–S3/41.
- Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1–187.
- Garland SM, Steben M. Genital warts. Best Pract Res Clin Obstet Gynaececol. 2014;28(7):1061–1073.
- Wiley DJ, Douglas J, Beutner K, et al. External genital warts: Diagnosis, treatment, and prevention. Clin Infect Dis. 2002;35(Suppl 2):S210–S224.
- Doorbar J, Quint W, Banks L, et al. The biology and life-cycle of human papillomaviruses. Vaccine. 2012;30(Suppl 5):F55–F70.
- Stanley M. HPV vaccination in boys and men. Hum Vaccin Immunother. 2014;10(7):2109–2111.
- Trottier H, Franco EL. The epidemiology of genital human papillomavirus infection. Vaccine. 2006;24(Suppl 1):S1/1–S1/15.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Year in Review: Chronic Lymphocytic Leukemia
2.
According to a study, white Americans are overdiagnosing melanoma at an alarming rate.
3.
Approval in Endometrial Cancer Expanded; Masks at Cancer Centers; NPR Reporter Dies
4.
The First Gene Therapy Provides a Durable Response for Non-Muscle-Invasive Bladder Cancer.
5.
Canine Cancer Vaccine: A Potential Resurrection? U.S. KK. Snubs Enertu.
1.
What Is Carboxyhemoglobin And How Can It Affect Your Health?
2.
Lu-177 Vipivotide in Prostate Cancer: A Breakthrough in Radioligand Therapy
3.
Unraveling the Mysteries of Coagulopathy: A Comprehensive Definition
4.
Machine Learning in Genomic Analysis for Early Lung Cancer Detection: Key Advances and Insights
5.
A New Perspective on Spherocytosis: Uncovering Innovative Treatments
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Revolutionizing Treatment of ALK Rearranged NSCLC with Lorlatinib - Part II
2.
Navigating the Complexities of Ph Negative ALL - Part XIII
3.
Updates on the First Line Management of ALK+ NSCLC
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
Breaking Ground: ALK-Positive Lung Cancer Front-Line Management - Part II

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge