Pelvic Inflammatory Disease: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Pelvic Inflammatory Disease (PID) is an infection of the upper female genital tract, involving the uterus, fallopian tubes, ovaries, and surrounding pelvic structures. It is most commonly caused by ascending infections, particularly Chlamydia trachomatis and Neisseria gonorrhoeae, although polymicrobial etiologies are frequently implicated. PID remains a major cause of reproductive morbidity worldwide, contributing significantly to infertility, ectopic pregnancy, and chronic pelvic pain.
We report the case of a 28-year-old sexually active female presenting with acute lower abdominal pain, fever, and abnormal vaginal discharge. Clinical findings, supported by laboratory and imaging investigations, were consistent with acute PID. The patient was treated with a combination of broad-spectrum antibiotics, resulting in rapid clinical improvement and complete resolution of symptoms on follow-up.
This case emphasizes the importance of early clinical suspicion, prompt initiation of empirical therapy, and comprehensive patient education to prevent long-term complications associated with PID.
Introduction
Pelvic Inflammatory Disease is a spectrum of inflammatory disorders of the upper female genital tract, including endometritis, salpingitis, tubo-ovarian abscess, and pelvic peritonitis. It predominantly affects women of reproductive age and represents a significant public health burden globally.
The incidence of PID is difficult to determine accurately due to underdiagnosis and variation in clinical presentation; however, it is estimated that millions of women are affected annually worldwide. The condition is strongly associated with sexually transmitted infections (STIs), particularly Chlamydia trachomatis and Neisseria gonorrhoeae. In many cases, endogenous vaginal flora, including anaerobes, Gardnerella vaginalis, and facultative organisms, contribute to a polymicrobial infection.
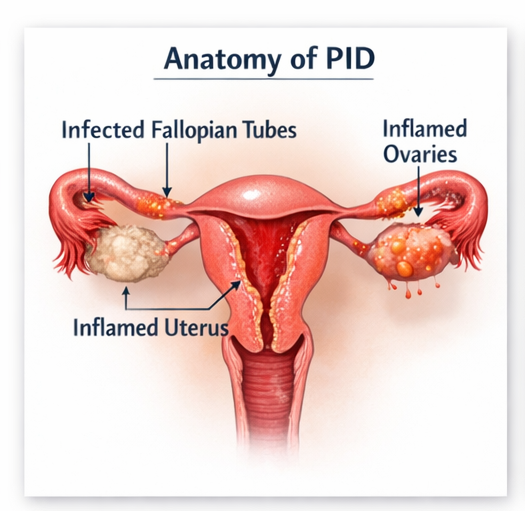
The pathogenesis involves ascending spread of microorganisms from the lower genital tract to the upper reproductive organs. This leads to inflammation, tissue destruction, and scarring, particularly affecting the fallopian tubes. These pathological changes can result in impaired fertility and increased risk of ectopic pregnancy.
Risk factors include:
• Multiple sexual partners
• Early onset of sexual activity
• Inconsistent condom use
• Previous history of PID or STIs
• Intrauterine device (IUD) insertion, especially shortly after placement
• Socioeconomic and behavioral factors
Clinical manifestations vary widely, ranging from mild, nonspecific symptoms to severe, life-threatening illness. Common symptoms include lower abdominal pain, fever, abnormal vaginal discharge, dyspareunia, and menstrual irregularities. However, many cases are subclinical, making early diagnosis challenging.
Case Report
Patient History
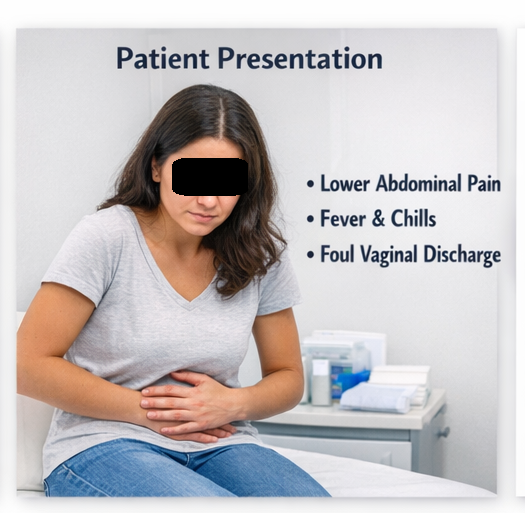
A 28-year-old female presented to the gynecology outpatient department with complaints of:
• Progressive lower abdominal pain for 5 days
• Fever associated with chills
• Foul-smelling vaginal discharge
• Pain during sexual intercourse (dyspareunia)
The pain was described as bilateral, dull aching, and exacerbated by movement. The patient reported a history of unprotected sexual intercourse with multiple partners over the past year. There was no history of recent surgical procedures, intrauterine device insertion, or known chronic medical conditions.
Menstrual history revealed irregular cycles over the previous two months. There was no history suggestive of ectopic pregnancy or prior episodes of PID.
Clinical Examination
On general examination:
• Temperature: 38.5°C
• Pulse: 102 beats per minute
• Blood pressure: 110/70 mmHg
Abdominal examination revealed lower abdominal tenderness without guarding or rigidity.
Pelvic examination demonstrated:
• Cervical motion tenderness (positive chandelier sign)
• Bilateral adnexal tenderness
• Purulent cervical discharge
No palpable adnexal mass was noted. The findings were highly suggestive of an inflammatory pelvic pathology.
Clinical Evaluation
Differential Diagnosis
Based on clinical presentation, the following conditions were considered:
• Pelvic inflammatory disease
• Ectopic pregnancy
• Acute appendicitis
• Ovarian torsion
• Endometriosis
The presence of fever, cervical motion tenderness, and abnormal discharge made PID the most likely diagnosis.
Investigations
Laboratory Findings
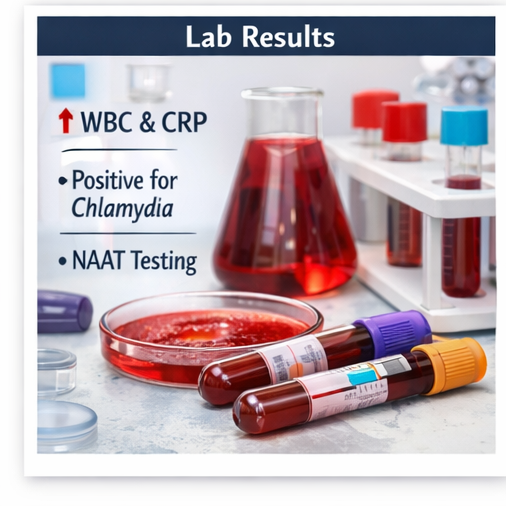
• Elevated white blood cell count indicating leukocytosis
• Increased C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR)
• Positive nucleic acid amplification test (NAAT) for Chlamydia trachomatis
• Negative urine pregnancy test
Microbiological Testing
Endocervical swab samples confirmed the presence of Chlamydia trachomatis, supporting the diagnosis of an STI-associated PID.
Imaging Studies
• Transvaginal ultrasound revealed:
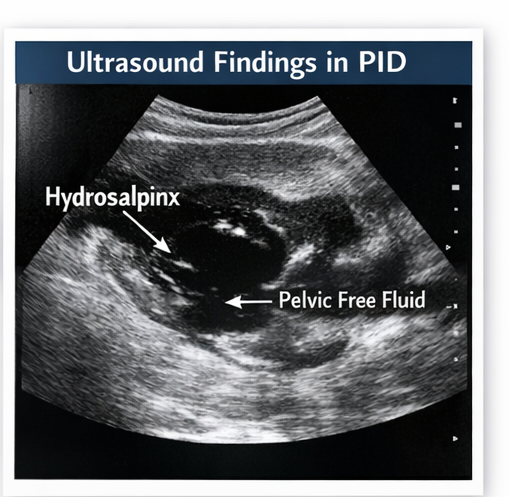
– Thickened, fluid-filled fallopian tubes (hydrosalpinx)
– Mild free fluid in the pelvis
– No evidence of tubo-ovarian abscess
• Doppler studies showed increased vascularity consistent with inflammation.
These imaging findings corroborated the clinical diagnosis of acute PID.
Diagnosis
Based on the clinical presentation, laboratory findings, and imaging studies, a diagnosis of acute pelvic inflammatory disease (salpingitis) was established.
Management and Outcome
Management Strategy
A multidisciplinary approach involving gynecology and infectious disease specialists was adopted. Early initiation of empirical antibiotic therapy was prioritized to prevent complications.
Primary Treatment
The patient was started on intravenous broad-spectrum antibiotics, including:

• Ceftriaxone (to cover Neisseria gonorrhoeae)
• Doxycycline (for Chlamydia trachomatis)
• Metronidazole (for anaerobic organisms)
This combination therapy ensured coverage of the polymicrobial etiology of PID.
Supportive Management
• Analgesics for pain control
• Intravenous fluids for hydration
• Counseling on safe sexual practices
• Partner notification and treatment to prevent reinfection
Follow-Up and Outcome
At 72 hours:
• Significant reduction in abdominal pain
• Resolution of fever
At 2 weeks:
• Complete resolution of vaginal discharge
• Marked improvement in pelvic tenderness
At 3 months:
• No recurrence of symptoms
• Patient counseled regarding fertility implications and preventive strategies
The patient demonstrated excellent clinical recovery with no immediate complications.
Discussion
Pathophysiology
PID occurs due to the ascent of pathogens from the lower genital tract to the upper reproductive organs. The infection triggers an inflammatory cascade, leading to:
• Edema and congestion of the fallopian tubes
• Formation of adhesions
• Tubal scarring and obstruction
These structural changes impair ovum transport, increasing the risk of infertility and ectopic pregnancy. Chronic inflammation may also result in persistent pelvic pain.
Diagnostic Challenges
The diagnosis of PID is primarily clinical and often challenging due to its variable presentation. Many patients present with mild or nonspecific symptoms, leading to underdiagnosis.
Key challenges include:
• Overlap with other abdominal and gynecological conditions
• Absence of definitive diagnostic tests
• Subclinical infections
Therefore, a low threshold for diagnosis and early empirical treatment is recommended in at-risk individuals.
Treatment Considerations
Antibiotic Therapy
Prompt initiation of broad-spectrum antibiotics is critical to prevent long-term sequelae. Treatment should cover common pathogens, including Chlamydia trachomatis, Neisseria gonorrhoeae, and anaerobes.
Hospitalization Criteria
Hospital admission is indicated in cases of:
• Severe clinical illness
• Pregnancy
• Suspected tubo-ovarian abscess
• Failure of outpatient therapy
• Diagnostic uncertainty
Complications
If left untreated or inadequately treated, PID can lead to serious complications:
• Infertility due to tubal damage
• Ectopic pregnancy
• Chronic pelvic pain
• Tubo-ovarian abscess
• Pelvic adhesions and peritonitis
Repeated episodes significantly increase the risk of long-term reproductive morbidity.
Prognosis
The prognosis of PID depends on the timing of diagnosis and initiation of treatment. Early intervention is associated with favorable outcomes, while delayed treatment increases the risk of irreversible complications.
Factors influencing prognosis include:
• Severity of infection
• Number of recurrent episodes
• Presence of complications
• Patient adherence to treatment
Conclusion
Pelvic Inflammatory Disease is a common yet potentially serious condition that requires prompt recognition and management. This case highlights the importance of early diagnosis based on clinical suspicion and supportive investigations.
Timely initiation of appropriate antibiotic therapy is essential to prevent complications such as infertility and chronic pelvic pain. A multidisciplinary approach, combined with patient education and preventive strategies, plays a crucial role in improving outcomes.
Routine screening for sexually transmitted infections and promotion of safe sexual practices are vital in reducing the overall burden of PID and its associated complications.
References
- Workowski, K. A., & Bolan, G. A. (2015). Sexually transmitted diseases treatment guidelines. MMWR Recommendations and Reports. https://pubmed.ncbi.nlm.nih.gov/26042815/
- Brunham, R. C., Gottlieb, S. L., & Paavonen, J. (2015). Pelvic inflammatory disease. New England Journal of Medicine. https://pubmed.ncbi.nlm.nih.gov/25607279/
- Haggerty, C. L., & Ness, R. B. (2006). Diagnosis and treatment of pelvic inflammatory disease. Women’s Health. https://pubmed.ncbi.nlm.nih.gov/17055377/
- Ross, J., et al. (2017). European guideline for the management of PID. International Journal of STD & AIDS. https://pubmed.ncbi.nlm.nih.gov/29161974/
- Wiesenfeld, H. C., & Sweet, R. L. (2013). Progress in PID management. Clinical Infectious Diseases. https://pubmed.ncbi.nlm.nih.gov/23315311/
- Walker, C. K., & Wiesenfeld, H. C. (2020). Antibiotic therapy for PID. Clinical Obstetrics and Gynecology. https://pubmed.ncbi.nlm.nih.gov/32483068/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge