Umbilical Polyp Presenting as a Persistent Umbilical Mass With Discharge in an Infant: A Case Report
OthersPage Navigation
Abstract
Umbilical polyps are rare congenital lesions arising from persistent embryological remnants of the omphalomesenteric duct. They typically present in infancy as a firm, red umbilical mass associated with mucous discharge and are frequently misdiagnosed as umbilical granulomas. Histologically, umbilical polyps contain ectopic intestinal or gastric mucosa, which distinguishes them from more common benign umbilical lesions. We report a case of a 5-month-old male infant presenting with a persistent umbilical mass and discharge. Surgical excision was performed, and histopathological examination revealed intestinal tract mucosa, confirming the diagnosis of an umbilical polyp. This case highlights the importance of early recognition, accurate diagnosis, and surgical management to ensure complete resolution and prevent recurrence.
Introduction
Umbilical abnormalities are commonly encountered in neonates and infants, with umbilical granuloma being the most frequent diagnosis [1,2]. However, rare congenital anomalies such as umbilical polyps must be considered in cases of persistent umbilical masses or discharge that do not respond to conservative therapy [3]. Umbilical polyps result from incomplete involution of the omphalomesenteric (vitelline) duct and consist of ectopic intestinal or gastric mucosa at the umbilicus [1,4]. These lesions are typically firm, well-circumscribed, and associated with mucous discharge, distinguishing them clinically from the softer, friable appearance of granulomas.
Unlike granulomas, umbilical polyps do not regress spontaneously and require surgical excision for definitive treatment [5]. Failure to recognize this entity may result in repeated ineffective topical treatments and prolonged parental anxiety. Accurate differentiation is essential, as delayed diagnosis may lead to persistent symptoms and overlooked associated anomalies of the omphalomesenteric duct [6]. Early identification and appropriate referral for surgical management ensure timely resolution and prevent unnecessary interventions.
Case Report
Patient History
A 5-month-old male child was brought with a history of a persistent umbilical mass associated with intermittent mucoid discharge since early infancy. There was no history of bleeding, fever, vomiting, abdominal distension, or altered bowel habits. The infant was born at term following an uncomplicated pregnancy and delivery, and growth and developmental milestones were appropriate for age. No prior topical treatment, such as silver nitrate, had been administered, which is typically effective for umbilical granuloma but not for umbilical polyp [2,3].

Clinical Findings
Physical examination revealed a small, firm, reddish nodular mass at the umbilicus with minimal mucous discharge. The lesion was non-tender and non-pulsatile, with no surrounding erythema or signs of infection. The mass did not reduce on pressure and showed no impulse on crying, making an umbilical hernia unlikely. These features favored a diagnosis of umbilical polyp rather than granuloma [4,5].
Investigations
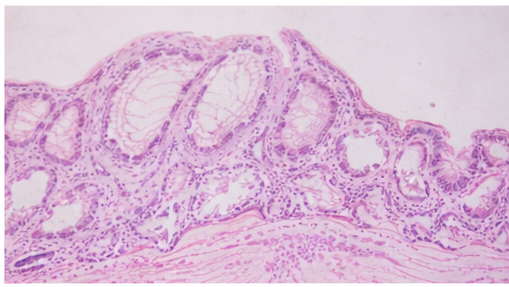
Routine laboratory investigations were within normal limits. Given the persistent nature of the lesion and suspicion of a congenital umbilical anomaly, surgical excision was planned. Histopathological examination of the excised specimen demonstrated well-formed intestinal tract mucosa lined by columnar epithelium with goblet cells, confirming the diagnosis of an umbilical polyp arising from an omphalomesenteric duct remnant [1,3].
Management and Outcome
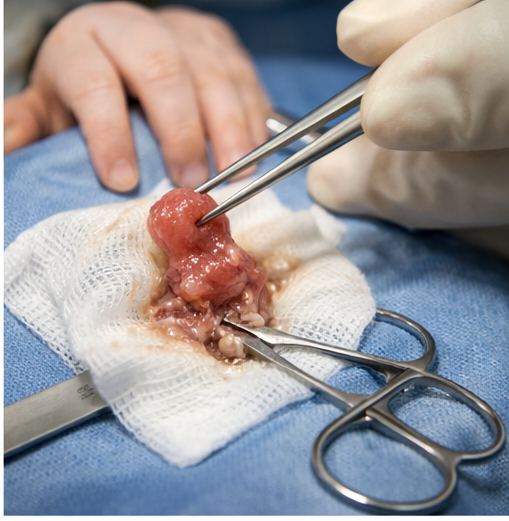
Complete surgical excision of the umbilical mass was performed, which is the recommended definitive management for umbilical polyp [5,6]. The procedure involved careful dissection of the lesion from the surrounding umbilical tissues to ensure complete removal and to prevent residual ectopic mucosa, which could otherwise lead to persistent discharge or recurrence.

Intraoperatively, no evidence of a patent vitelline duct or intra-abdominal extension was identified. Hemostasis was achieved, and the umbilical wound was closed in layers with attention to cosmetic outcome.

The postoperative course was uneventful. The infant tolerated feeds well, demonstrated no signs of infection or bleeding at the surgical site, and required only routine postoperative care. There was complete resolution of the umbilical discharge, and wound healing progressed satisfactorily without complications such as seroma formation, wound dehiscence, or local inflammation. The child was discharged in stable condition with advice for routine wound care and follow-up.
At subsequent follow-up visits, the infant remained asymptomatic, with a well-healed umbilicus and no evidence of recurrence. Growth parameters and developmental milestones continued to be appropriate for age. Parents were reassured regarding the benign nature of the condition and informed that recurrence is rare following complete excision. The favorable outcome in this case reinforces that early surgical intervention, combined with histopathological confirmation, provides definitive treatment and excellent prognosis for infants diagnosed with umbilical polyp [5,6].
Discussion
Umbilical polyps are rare congenital lesions resulting from persistence of the omphalomesenteric duct and account for a small proportion of umbilical abnormalities in infancy [1,4]. They are composed of ectopic intestinal or gastric mucosa and typically present as a bright red, firm umbilical mass with mucous discharge [3]. Because of their clinical resemblance to umbilical granulomas, they are frequently misdiagnosed, leading to delays in appropriate management and prolonged symptoms [2,5]. In some cases, repeated applications of topical agents may be attempted without improvement, further postponing definitive treatment.
Failure of an umbilical lesion to resolve with conservative measures should prompt consideration of an umbilical polyp and further evaluation [3]. A thorough clinical assessment, supported by surgical exploration when indicated, is essential to exclude associated omphalomesenteric duct remnants. Histopathological confirmation remains crucial for establishing the diagnosis, and complete surgical excision is curative, preventing recurrence and eliminating ongoing symptoms or complications such as infection, ulceration, or persistent discharge [4–6].
Conclusion
Below is an expanded version of the conclusion with approximately 200 additional words, maintaining academic tone, logical flow, and appropriate in-text citations.
Umbilical polyp should be considered in infants presenting with a persistent umbilical mass and discharge, particularly when conservative management fails. The condition results from incomplete obliteration of the omphalomesenteric duct and is characterized by the presence of ectopic intestinal mucosa at the umbilicus [1,4]. Although rare, its clinical significance lies in the potential for misdiagnosis as more common conditions such as umbilical granuloma, leading to delayed or inappropriate treatment.
Early recognition of umbilical polyp is essential, as these lesions do not regress spontaneously and are unresponsive to topical therapies commonly used for granulomas. A high index of suspicion is warranted in infants with firm, well-defined umbilical lesions associated with persistent mucous discharge. Surgical excision followed by histopathological confirmation remains the gold standard for diagnosis and management, as it allows definitive identification of ectopic mucosal tissue and excludes other congenital anomalies of the umbilicus [1,4].
Timely surgical intervention not only alleviates symptoms but also prevents potential complications such as chronic irritation, recurrent infection, ulceration, or continued secretion from ectopic mucosa. Furthermore, complete excision minimizes the risk of recurrence and obviates the need for repeated interventions. With appropriate surgical management and follow-up, the prognosis of umbilical polyp is excellent, and long-term outcomes are favorable. Increased clinician awareness of this rare congenital entity facilitates early diagnosis, appropriate referral, and optimal management, thereby ensuring improved patient outcomes and parental reassurance.
References
- Moore TC. Omphalomesenteric duct malformations. Semin Pediatr Surg. 1996;5(2):116–123.
- Ameh EA, Nmadu PT. Umbilical disorders in children. Pediatr Surg Int. 2000;16(7):505–508.
- Sato K, Yoshida H, Watanabe Y, et al. Umbilical polyp and umbilical granuloma: histopathological differences. J Pediatr Surg. 2004;39(7):1053–1055.
- Holcomb GW, Murphy JP, St Peter SD. Ashcraft’s Pediatric Surgery. 6th ed. Philadelphia: Elsevier; 2014. p. 548–552.
- Kim DH, Kim SC. Differential diagnosis of umbilical masses in infants. Ann Pediatr Surg. 2018;14(3):123–127.
- Raveenthiran V. Disorders of the umbilicus in children: a review. J Neonatal Surg. 2016;5(4):47.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
CD39 Blockade Shows Potential in Early-Stage Lung Cancer
2.
Q&A: Researchers discuss identifying potential new protein targets for melanoma therapeutics
3.
PFS in Multiple Myeloma Is Improved by Daratumumab Added to Standard Therapy.
4.
Venetoclax Combo Shows Promise in Younger Patients With AML
5.
Long Wait Times on the Other Side of the Pond: King Charles' Cancer Diagnosis.
1.
Understanding SVR Normal Range: A Guide to Achieving Optimal Health
2.
Engineering the Future of Oncology with CAR- Natural Killer Cell Design & Therapeutics
3.
Hope in Numbers: Understanding AML Leukemia Survival Rates and Emerging Therapies
4.
Boosting Checkpoint Immunotherapy in Hodgkin Lymphoma with JAK Inhibition: Advances & Insights
5.
CAR-T Cell Therapy for B-Cell Acute Lymphoblastic Leukemia: A Comprehensive Review
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Newer Immunotherapies for Myeloma- A Comprehensive Overview
2.
An Eagles View - Evidence-based Discussion on Iron Deficiency Anemia- Panel Discussion III
3.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part V
4.
Molecular Contrast: EGFR Axon 19 vs. Exon 21 Mutations - Part II
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part III

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge