Cushing’s Syndrome: Diagnostic Challenges and Clinical Management - A Case Report
OthersPage Navigation
Abstract
Cushing’s syndrome is a rare but clinically significant endocrine disorder resulting from chronic exposure to excessive glucocorticoids. Its presentation is often insidious and heterogeneous, frequently mimicking more common metabolic and cardiovascular conditions. Early recognition is critical, as prolonged hypercortisolism is associated with substantial morbidity and increased mortality. We report a case of endogenous Cushing’s syndrome in a middle-aged woman who presented with progressive weight gain, poorly controlled hypertension, and diabetes mellitus. Comprehensive biochemical evaluation and targeted imaging confirmed the diagnosis of an adrenocorticotropic hormone (ACTH)-dependent Cushing’s syndrome secondary to a pituitary adenoma. This case highlights the importance of clinical suspicion, systematic diagnostic evaluation, and multidisciplinary management in optimizing outcomes for patients with Cushing’s syndrome.
Introduction
Cushing’s syndrome encompasses a constellation of clinical features caused by prolonged exposure to elevated levels of cortisol, either endogenous or exogenous in origin. Although exogenous corticosteroid use remains the most common cause, endogenous Cushing’s syndrome is rare, with an estimated annual incidence of 1–3 cases per million population [1]. Despite its rarity, the condition carries significant clinical importance due to its association with cardiovascular disease, metabolic derangements, osteoporosis, immunosuppression, and increased mortality.
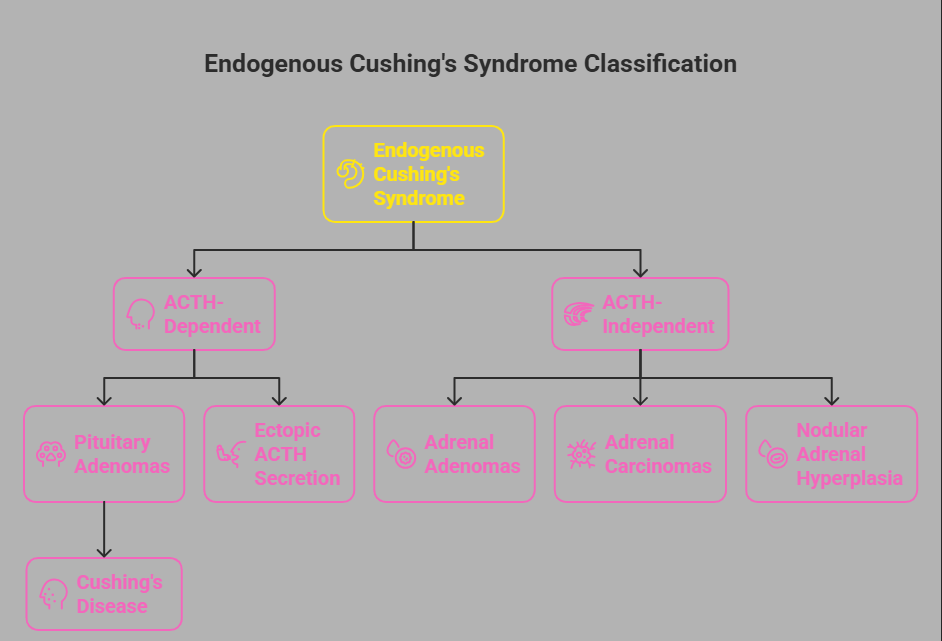
Endogenous Cushing’s syndrome is broadly classified into ACTH-dependent and ACTH-independent forms. ACTH-dependent causes include pituitary adenomas (Cushing’s disease) and ectopic ACTH secretion, whereas ACTH-independent causes primarily arise from adrenal adenomas, carcinomas, or nodular adrenal hyperplasia [2]. The clinical presentation is often subtle in early stages, leading to diagnostic delays that may span several years.
This case report describes a patient with ACTH-dependent Cushing’s syndrome, emphasizing the diagnostic complexity, the role of biochemical and radiological investigations, and the principles guiding clinical management.
Case Report
Patient History
A 42-year-old woman was referred to the endocrinology clinic with complaints of progressive weight gain, fatigue, and menstrual irregularities over the preceding 18 months. She reported a gradual increase in central adiposity despite no significant change in dietary habits. Over the same period, she experienced worsening facial rounding, easy bruising, proximal muscle weakness, and new-onset acne.
Her medical history was notable for hypertension diagnosed one year earlier and type 2 diabetes mellitus diagnosed six months prior, both of which were poorly controlled despite escalating pharmacological therapy. There was no history of exogenous corticosteroid use, including oral, inhaled, topical, or injectable preparations. She denied symptoms suggestive of depression or alcohol misuse. There was no family history of endocrine disorders.
Clinical Findings
On physical examination, the patient appeared overweight with a body mass index of 31 kg/m². She exhibited classical cushingoid features, including moon facies, supraclavicular fat pads, and truncal obesity with relatively thin extremities. Blood pressure was elevated at 156/98 mmHg despite antihypertensive therapy.

Cutaneous examination revealed wide, violaceous striae over the abdomen and thighs, along with multiple ecchymoses on the upper limbs. Proximal muscle weakness was evident, particularly involving the hip girdle muscles. Facial acne and mild hirsutism were noted. No features of virilization or hyperpigmentation were present. Cardiovascular, respiratory, and neurological examinations were otherwise unremarkable.
Investigations
Initial Laboratory Evaluation
Baseline laboratory investigations demonstrated persistent hyperglycemia with elevated fasting plasma glucose and glycated hemoglobin levels. Serum electrolytes revealed mild hypokalemia. Complete blood counts showed leukocytosis with neutrophilic predominance, consistent with cortisol-induced immune modulation.
Given the constellation of clinical features suggestive of hypercortisolism, screening tests for Cushing’s syndrome were performed. A 24-hour urinary free cortisol level was markedly elevated on two separate collections, exceeding three times the upper limit of normal. Late-night salivary cortisol levels were also significantly elevated, indicating loss of normal diurnal cortisol variation.
Confirmatory Testing
A low-dose overnight dexamethasone suppression test failed to suppress morning serum cortisol levels, further confirming endogenous hypercortisolism. Plasma ACTH measurement revealed inappropriately normal to elevated ACTH levels, suggesting an ACTH-dependent etiology.
To differentiate between pituitary and ectopic sources of ACTH secretion, a high-dose dexamethasone suppression test was performed. Partial suppression of serum cortisol levels was observed, favoring a pituitary source. Magnetic resonance imaging (MRI) of the pituitary gland subsequently revealed a 6-mm hypoenhancing lesion consistent with a pituitary microadenoma.
Inferior petrosal sinus sampling was considered but deferred, given the concordant biochemical and radiological findings strongly suggestive of Cushing’s disease.
Diagnosis
Based on clinical presentation, biochemical confirmation of hypercortisolism, elevated ACTH levels, partial suppression on high-dose dexamethasone testing, and pituitary imaging findings, a diagnosis of ACTH-dependent Cushing’s syndrome due to a pituitary adenoma (Cushing’s disease) was established.
Management and Outcome
The patient was managed through a multidisciplinary approach involving endocrinology, neurosurgery, and anesthesiology teams. Preoperative optimization included stringent glycemic control, correction of hypokalemia, and management of hypertension. Medical therapy with a steroidogenesis inhibitor was initiated temporarily to reduce cortisol levels and minimize perioperative risk.

She subsequently underwent transsphenoidal surgical resection of the pituitary adenoma. The procedure was uneventful, and histopathological examination confirmed an ACTH-secreting pituitary adenoma.

Postoperatively, the patient developed transient adrenal insufficiency, necessitating short-term glucocorticoid replacement therapy, which was gradually tapered under close endocrinological supervision. Over the following months, she demonstrated significant clinical improvement, with reduction in facial rounding, gradual weight loss, improved muscle strength, and resolution of skin changes.
Her blood pressure and glycemic control improved substantially, allowing de-escalation of antihypertensive and antidiabetic medications. Follow-up biochemical testing revealed normalization of cortisol levels, and repeat imaging showed no evidence of residual or recurrent disease.
Discussion
Cushing’s syndrome remains a diagnostic challenge due to its variable presentation and overlap with common metabolic disorders such as obesity, diabetes, and hypertension. Delayed diagnosis is associated with increased cardiovascular risk, osteoporosis, psychiatric morbidity, and infections [3].
This case underscores the importance of maintaining a high index of suspicion in patients with progressive metabolic abnormalities and characteristic physical features. Screening tests such as urinary free cortisol, late-night salivary cortisol, and dexamethasone suppression testing are essential initial tools, but results must be interpreted within the broader clinical context [4].
ACTH-dependent Cushing’s syndrome accounts for approximately 80% of endogenous cases, with pituitary adenomas being the most common cause. Differentiating pituitary from ectopic ACTH secretion is crucial, as management strategies differ significantly. High-dose dexamethasone testing, pituitary imaging, and inferior petrosal sinus sampling remain cornerstone investigations in challenging cases [5].
Surgical resection of the causative lesion remains the treatment of choice for Cushing’s disease. However, long-term follow-up is essential due to the risk of recurrence and the potential for persistent comorbidities despite biochemical remission. Early diagnosis and intervention are key determinants of long-term prognosis and quality of life.
Conclusion
Cushing’s syndrome is a complex endocrine disorder with significant systemic implications if left untreated. This case highlights the critical role of thorough clinical assessment, structured biochemical testing, and targeted imaging in achieving an accurate diagnosis.
Timely, individualized management through a multidisciplinary approach can lead to favorable outcomes, including reversal of metabolic complications and improved quality of life. Increased awareness and early recognition of Cushing’s syndrome are essential to reduce diagnostic delays and mitigate long-term morbidity associated with chronic hypercortisolism.
References
- Nieman LK, et al. The diagnosis of Cushing’s syndrome: An Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2008;93(5):1526–1540.
- Newell-Price J, et al. Cushing’s syndrome. Lancet. 2006;367(9522):1605–1617.
- Pivonello R, et al. Complications of Cushing’s syndrome: State of the art. Lancet Diabetes Endocrinol. 2016;4(7):611–629.
- Arnaldi G, et al. Diagnosis and complications of Cushing’s syndrome: A consensus statement. J Clin Endocrinol Metab. 2003;88(12):5593–5602.
- Oldfield EH, et al. Petrosal sinus sampling with and without CRH stimulation in the differential diagnosis of Cushing’s syndrome. N Engl J Med. 1991;325(13):897–905.
- Fleseriu M, et al. Management of Cushing’s disease: Current therapy and future directions. Endocr Rev. 2022;43(2):225–252.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Potential targets for treating the most common type of liver cancer in children have been identified by a collaborative study.
2.
Study identifies new approach to protect the brain during radiation therapy
3.
While most cancer screenings won't prolong lives, there are still good reasons to continue screening.
4.
Chemo-Free Quadruplet Shows Promise as DLBCL's First Therapy.
5.
Radiation therapy for patients with breast cancer
1.
Radiation in Oncology: Advances, Applications, and Accessibility
2.
The Next Generation of Precision: How Multi-Specific Antibodies are Redefining Oncology's Future - A 2025 Review
3.
Cracking Oncology Drug Resistance: New Strategies to Overcome Challenges in Modern Cancer Therapy
4.
Unlocking the Secrets of Neutrophils: Exploring Their Role in Immune Defense
5.
Precision Oncology: Personalized Medicine Shaping the Future of Cancer Care
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Pazopanib Takes Center Stage in Managing Renal Cell Carcinoma - Part II
2.
Recent Data Analysis for First-Line Treatment of ALK+ NSCLC
3.
Navigating the Complexities of Ph Negative ALL - Part XIII
4.
Navigating the Complexities of Ph Negative ALL - Part IV
5.
Revolutionizing Treatment of ALK Rearranged NSCLC with Lorlatinib - Part VIII

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge