Macular Detachment: Diagnostic Evaluation, Surgical Management, and Visual Outcome - A Case Report
OthersPage Navigation
Abstract
Macular detachment represents a vision-threatening manifestation of retinal pathology, most commonly occurring in the context of rhegmatogenous retinal detachment. Involvement of the macula is a critical prognostic determinant, as prolonged separation of the neurosensory retina from the retinal pigment epithelium results in irreversible photoreceptor damage and suboptimal visual recovery. Early diagnosis, accurate assessment of macular status, and timely surgical intervention are essential to preserve central vision. We report a case of macula-off retinal detachment in a middle-aged male presenting with acute visual impairment. Comprehensive ophthalmic examination, multimodal retinal imaging, and prompt vitreoretinal surgery resulted in successful anatomical reattachment and meaningful visual improvement. This case highlights the importance of early symptom recognition, structured diagnostic evaluation, and evidence-based surgical management in optimizing outcomes for patients with macular detachment.
Introduction
Macular detachment refers to the involvement of the macula in retinal detachment, leading to significant impairment of central vision and visual acuity. Rhegmatogenous retinal detachment (RRD), caused by a full-thickness retinal break allowing liquefied vitreous to enter the subretinal space, is the most common etiology [1]. Other causes include tractional retinal detachment, exudative retinal detachment, and vitreomacular interface disorders.
The macula is responsible for high-resolution central vision, and its detachment initiates a cascade of cellular and metabolic changes, including photoreceptor apoptosis, disruption of the outer retinal layers, and altered retinal pigment epithelium function [2]. Clinical studies have consistently shown that both the duration and extent of macular detachment significantly influence postoperative visual outcomes [3].
Advances in diagnostic imaging, particularly optical coherence tomography (OCT), have enhanced the clinician’s ability to assess macular involvement and predict visual prognosis. Similarly, improvements in vitreoretinal surgical techniques, including pars plana vitrectomy and internal tamponade agents, have improved anatomical success rates. Despite these advances, macula-off retinal detachment remains a challenge, emphasizing the importance of early diagnosis and intervention. This case report describes the clinical presentation, diagnostic evaluation, and multidisciplinary management of macular detachment, illustrating key principles of contemporary retinal care.
Case Report
Patient History
A 52-year-old male presented to the ophthalmology outpatient department with a sudden, painless decrease in vision in the right eye for five days. The visual disturbance was preceded by intermittent flashes of light and the sudden appearance of multiple floaters. Over the subsequent days, the patient noticed a dark shadow progressing from the peripheral field toward the center of vision.
The patient had a history of moderate myopia for over two decades and controlled systemic hypertension managed with oral antihypertensive therapy. There was no history of diabetes mellitus, ocular trauma, previous ocular surgery, or inflammatory eye disease. Family history was unremarkable for retinal disorders.
Clinical Examination
On examination, the patient was alert and cooperative. Best-corrected visual acuity (BCVA) in the right eye was counting fingers at 2 meters, while the left eye had a BCVA of 6/6. Pupillary reactions were normal, with no relative afferent pupillary defect.

Anterior segment examination of both eyes revealed a clear cornea, normal anterior chamber depth, and clear crystalline lens. Intraocular pressure measured by applanation tonometry was within normal limits in both eyes.
Dilated fundus examination of the right eye revealed a bullous retinal detachment involving the posterior pole, with clear elevation of the macula. A horseshoe-shaped retinal tear was identified in the superotemporal quadrant, with surrounding lattice degeneration. The left eye fundus examination was unremarkable.
Investigations
Optical Coherence Tomography (OCT)
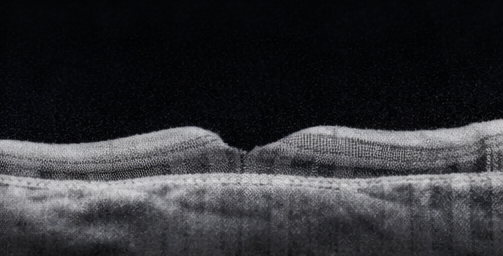
Spectral-domain OCT of the right eye confirmed macular detachment with accumulation of subretinal fluid beneath the fovea and loss of normal foveal contour.

The outer retinal layers showed early disruption of the ellipsoid zone, suggestive of photoreceptor stress without established atrophy. OCT imaging of the left eye was normal.

Ultrasonography (B-scan)
B-scan ultrasonography demonstrated a mobile, undulating retinal membrane consistent with rhegmatogenous retinal detachment. No vitreous hemorrhage, choroidal detachment, or intraocular mass was identified.
Diagnosis
Based on the clinical presentation, fundus findings, and multimodal imaging, a diagnosis of macula-off rhegmatogenous retinal detachment involving the right eye was established. The relatively short duration of macular involvement supported an urgent surgical approach to maximize the potential for visual recovery.
Management and Outcome
Multidisciplinary Care
The patient was counseled by a vitreoretinal specialist regarding the nature of the condition, prognosis, and treatment options. After informed consent, surgical repair was planned on an urgent basis.
Surgical Management
The patient underwent pars plana vitrectomy with endolaser photocoagulation and sulfur hexafluoride (SF6) gas tamponade under local anesthesia. Intraoperatively, complete removal of the vitreous gel was achieved, relieving vitreoretinal traction. The retinal tear was identified and surrounded with laser photocoagulation. Subretinal fluid was drained, and the retina was successfully reattached.

Postoperatively, the patient was advised strict prone positioning for seven days to ensure optimal gas tamponade of the retinal break. Topical antibiotics, corticosteroids, and cycloplegic agents were prescribed.
Follow-Up and Outcome
At one-week follow-up, fundus examination confirmed complete retinal reattachment with gradual absorption of intraocular gas. OCT imaging at four weeks demonstrated resolution of subretinal fluid and partial restoration of the foveal architecture.
At three-month follow-up, BCVA in the right eye improved to 6/18. The patient reported marked improvement in central vision, although mild metamorphopsia persisted. The retina remained anatomically attached, and OCT showed continued improvement in outer retinal integrity.
Discussion
Macular detachment remains one of the most significant predictors of poor visual outcome in retinal detachment. Experimental studies have demonstrated that photoreceptor degeneration begins shortly after macular separation, with increasing duration leading to irreversible damage [4].
OCT has emerged as an indispensable tool in evaluating macular involvement, providing insights into photoreceptor integrity and enabling postoperative monitoring. Restoration of the ellipsoid zone on OCT correlates strongly with visual recovery [5].
Pars plana vitrectomy has become the preferred surgical approach for macula-off retinal detachments, particularly in cases with posterior breaks, extensive detachment, or vitreous traction. While anatomical success rates exceed 90%, visual outcomes remain variable and depend on factors such as duration of macular detachment, patient age, and preoperative visual acuity.
This case highlights the importance of early symptom recognition and patient education. Prompt referral following the onset of flashes, floaters, or visual field defects can significantly improve outcomes.
Conclusion
Macular detachment is a sight-threatening ophthalmic emergency requiring timely diagnosis and urgent surgical management. This case demonstrates that early vitreoretinal intervention, guided by detailed clinical assessment and advanced imaging, can achieve favorable anatomical reattachment and meaningful visual recovery. Ongoing patient education, early referral, and advances in surgical techniques remain central to improving outcomes in macula-off retinal detachment.
References
-
Mitry D, et al. The epidemiology of rhegmatogenous retinal detachment. Ophthalmology. 2010;117(2):354–360.
-
Ross WH, Kozy DW. Visual recovery in macula-off retinal detachments. Ophthalmology. 1998;105(11):2149–2153.
-
Wickham L, et al. Surgical outcomes of macula-off retinal detachment. Eye. 2004;18(7):666–671.
-
Cook B, Lewis GP, Fisher SK, Adler R. Apoptotic photoreceptor degeneration in experimental retinal detachment. Invest Ophthalmol Vis Sci. 1995;36(5):990–996.
-
Steel DHW. Retinal detachment surgery: Current practice and future directions. Eye. 2020;34(9):1651–1662.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Year in Review: Chronic Lymphocytic Leukemia
2.
According to a study, white Americans are overdiagnosing melanoma at an alarming rate.
3.
Approval in Endometrial Cancer Expanded; Masks at Cancer Centers; NPR Reporter Dies
4.
The First Gene Therapy Provides a Durable Response for Non-Muscle-Invasive Bladder Cancer.
5.
Canine Cancer Vaccine: A Potential Resurrection? U.S. KK. Snubs Enertu.
1.
What Is Carboxyhemoglobin And How Can It Affect Your Health?
2.
Lu-177 Vipivotide in Prostate Cancer: A Breakthrough in Radioligand Therapy
3.
Unraveling the Mysteries of Coagulopathy: A Comprehensive Definition
4.
Machine Learning in Genomic Analysis for Early Lung Cancer Detection: Key Advances and Insights
5.
A New Perspective on Spherocytosis: Uncovering Innovative Treatments
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Revolutionizing Treatment of ALK Rearranged NSCLC with Lorlatinib - Part II
2.
Navigating the Complexities of Ph Negative ALL - Part XIII
3.
Updates on the First Line Management of ALK+ NSCLC
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
Breaking Ground: ALK-Positive Lung Cancer Front-Line Management - Part II

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge