Brucellosis Presenting with Undulant Fever and Arthritis in a Veterinarian: A Case Report
OthersPage Navigation
Abstract
Brucellosis is a zoonotic bacterial infection caused by Brucella species and remains an important public health concern in endemic regions. Humans acquire the infection through direct contact with infected animals or consumption of unpasteurized dairy products. We report a case of brucellosis in a 32-year-old veterinarian who presented with undulant fever, malaise, and inflammatory arthritis following consumption of unpasteurized milk. Serological testing using the Standard Agglutination Test (SAT) and enzyme-linked immunosorbent assay (ELISA) confirmed the diagnosis, with the likely etiologic agent being Brucella melitensis or Brucella abortus. Prompt initiation of combination antibiotic therapy resulted in clinical improvement. This case underscores the importance of occupational risk assessment, dietary history, and early serologic testing in patients with prolonged fever and musculoskeletal symptoms.
Introduction
Brucellosis is a systemic zoonotic infection caused by gram-negative, facultative intracellular coccobacilli of the genus Brucella. The most common species causing human disease include Brucella melitensis, Brucella abortus, Brucella suis, and Brucella canis, with B. melitensis being associated with the most severe clinical manifestations due to its higher virulence and propensity for systemic involvement [1,2]. Despite sustained global control efforts, including livestock vaccination programs and food safety regulations, brucellosis remains endemic in many regions of Asia, the Middle East, Africa, and Latin America, where it continues to pose a significant public health challenge [3]. Socioeconomic factors, traditional animal husbandry practices, and widespread consumption of unpasteurized dairy products contribute to the persistent transmission of this infection.
Humans typically acquire infection through ingestion of unpasteurized milk or dairy products, inhalation of contaminated aerosols, or direct contact with infected animals and animal tissues, particularly during parturition or slaughter.

As a result, veterinarians, farmers, abattoir workers, and laboratory personnel are at particularly high risk of occupational exposure [2,4]. Following entry into the human host, Brucella organisms localize within macrophages, allowing them to evade host immune defenses and disseminate to multiple organ systems, accounting for the chronicity and relapsing nature of the disease.
Clinically, brucellosis is characterized by protean and often nonspecific manifestations, frequently leading to diagnostic delay or misdiagnosis. Common presenting features include undulant fever, night sweats with a characteristic foul odor, profound fatigue, malaise, arthralgia, and weight loss. Osteoarticular involvement is the most frequent focal complication and may present as arthritis, sacroiliitis, or spondylitis, significantly contributing to morbidity [5]. Given these variable presentations, a high index of clinical suspicion is essential, particularly in individuals with relevant occupational or dietary exposure.
We describe a case of occupationally acquired brucellosis in a veterinarian, highlighting the importance of thorough exposure history, appropriate serological testing, and timely initiation of combination antimicrobial therapy to prevent chronic disease and long-term complications.
Case Report
Patient History
A 32-year-old male veterinarian presented to the outpatient department with a 3-week history of intermittent fever, profound fatigue, generalized malaise, and progressive joint pain. The fever was described as undulating, with evening spikes associated with chills and drenching night sweats. He also reported loss of appetite and myalgia.

The patient worked in a rural veterinary practice with frequent exposure to cattle, sheep, and goats. He admitted to regular consumption of unpasteurized milk obtained from local farms. There was no history of recent travel, tuberculosis exposure, or chronic medical illness.
Clinical Findings
On examination, the patient was febrile (38.5°C) and appeared fatigued. Musculoskeletal examination revealed tenderness and restricted movement of the right knee and left ankle, consistent with inflammatory arthritis. No joint deformities were noted. Mild hepatosplenomegaly was appreciated on abdominal examination. There was no lymphadenopathy, rash, or neurological deficit.
Based on the occupational exposure, dietary history, undulant fever, and arthritis, a provisional diagnosis of brucellosis was considered.
Investigations
Laboratory investigations revealed mild anemia and leukopenia, with elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Liver function tests showed mild transaminitis. Blood cultures were obtained but remained sterile.
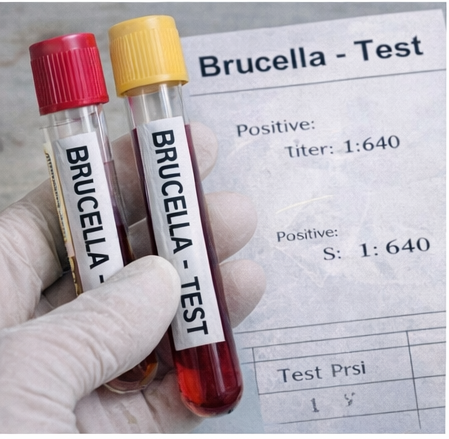
Serological testing demonstrated a positive Standard Agglutination Test (SAT) with a titer of 1:640, which is diagnostic in the appropriate clinical context. ELISA revealed elevated anti-Brucella IgM and IgG antibodies, confirming active infection. The findings were consistent with brucellosis, most likely caused by Brucella melitensis or Brucella abortus, given the exposure history.

Management and Outcome
The patient was started on combination antibiotic therapy consisting of doxycycline (100 mg twice daily) and rifampicin (600 mg once daily) for a planned duration of six weeks, in accordance with World Health Organization recommendations. Nonsteroidal anti-inflammatory drugs were prescribed for symptomatic relief of arthritis.
Within two weeks of therapy, the patient became afebrile, and joint pain significantly improved. At completion of treatment, inflammatory markers normalized, and the patient reported complete resolution of symptoms. No relapse was noted at three-month follow-up.
Discussion
Brucellosis is often referred to as “the great imitator” due to its wide range of nonspecific clinical manifestations, which frequently lead to delayed or missed diagnoses [3,5]. Occupational exposure remains a major risk factor, and veterinarians are among the highest-risk groups due to frequent contact with infected animals and animal products [4].
Undulant fever and osteoarticular involvement are hallmark features of brucellosis. Arthritis, sacroiliitis, and spondylitis represent the most common focal complications and may dominate the clinical presentation [6]. Consumption of unpasteurized milk remains a critical route of transmission, particularly in endemic regions where traditional dietary practices persist.
Serological tests such as SAT and ELISA remain the cornerstone of diagnosis, especially when blood cultures are negative or unavailable. ELISA provides added value by differentiating acute from chronic infection through IgM and IgG detection [2,7]. Early diagnosis is essential, as delayed treatment increases the risk of chronic disease, relapse, and complications.
Combination antibiotic therapy is required due to the intracellular nature of Brucella species. Doxycycline-based regimens combined with rifampicin or aminoglycosides have demonstrated high efficacy and reduced relapse rates [1,6].
Conclusion
Brucellosis should be considered in patients presenting with prolonged undulant fever, malaise, and arthritis, particularly in those with occupational exposure to livestock or a history of consuming unpasteurized dairy products. The nonspecific and often insidious nature of symptoms frequently leads to delayed diagnosis, especially in non-endemic settings or when occupational history is not adequately explored. Clinicians should maintain a high index of suspicion in patients with fever of unknown origin, musculoskeletal complaints, or systemic symptoms that do not respond to standard empirical therapies, as early recognition is critical to preventing disease progression.
A thorough exposure history, including occupational risks, dietary habits, and contact with animals or animal products, combined with appropriate serological testing such as the Standard Agglutination Test and enzyme-linked immunosorbent assay, is essential for establishing an early and accurate diagnosis. In selected cases, blood cultures and imaging studies may further aid in identifying focal complications, particularly osteoarticular or visceral involvement. Early diagnosis not only facilitates prompt treatment but also reduces the risk of transmission and long-term morbidity.
Prompt initiation of combination antibiotic therapy, tailored to disease severity and focal involvement, leads to excellent clinical outcomes and significantly reduces relapse rates. Delayed or inadequate treatment may result in chronic brucellosis, characterized by persistent symptoms, functional impairment, and reduced quality of life. Increased awareness among clinicians, particularly those practicing in endemic areas, is therefore essential. Equally important is education of at-risk populations regarding preventive measures, including avoidance of unpasteurized dairy products and adherence to occupational safety practices. Strengthening surveillance, early reporting, and preventive strategies can collectively reduce disease burden and improve overall public health outcomes.
References
- Pappas G, Akritidis N, Bosilkovski M, Tsianos E. Brucellosis. New England Journal of Medicine. 2005;352(22):2325–2336.
- Corbel MJ. Brucellosis in humans and animals. World Health Organization; 2006.
- Franco MP, Mulder M, Gilman RH, Smits HL. Human brucellosis. The Lancet Infectious Diseases. 2007;7(12):775–786.
- Young EJ. An overview of human brucellosis. Clinical Infectious Diseases. 1995;21(2):283–289.
- Colmenero JD, Reguera JM, Martos F, et al. Complications associated with Brucella melitensis infection: a study of 530 cases. Medicine (Baltimore). 1996;75(4):195–211.
- Solera J, Martínez-Alfaro E, Espinosa A. Recognition and optimum treatment of brucellosis. Drugs. 1997;53(2):245–256.
- Mantur BG, Amarnath SK. Brucellosis in India – a review. Journal of Biosciences. 2008;33(4):539–547.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Psychedelic Therapy Tied to Reduced Depression, Anxiety.
2.
New drug resistance mechanism in melanoma leptomeningeal disease revealed by study.
3.
Research finds stark disparities in treatment and survival time for people with pancreatic cancer
4.
Tumor characteristics found to differ for melanomas in children, teens and young adults
5.
Relationship-building key to addressing oncologist shortages in rural care
1.
Artificial Intelligence in Oncology: Current Trends, Challenges and Future Outlook
2.
Colon cancer: Risk factors, warning signs and treatment options
3.
Exploring the Latest Advances in Hodgkin's Lymphoma Treatment
4.
Can We Repurpose BV-CHP for Better Outcomes in Peripheral T-Cell Lymphoma?
5.
The Expanding Horizon of PSMA: A Comparative Clinical Review of Theranostics in Prostate Cancer and Beyond
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Navigating the Brain Barrier: The CNS Challenge in ALK+ NSCLC
2.
Efficient Management of First line ALK-rearranged NSCLC - Part VIII
3.
Evolution in Treatment and Diagnosis of Lung Cancer- An Initiative from Manipal Hospitals
4.
Molecular Contrast: EGFR Axon 19 vs. Exon 21 Mutations - Part V
5.
INO-VATE: The Long-Term Overall Survival Analysis in Iontuzumab-Treated Patients

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge