Lipoma: Clinical Evaluation, Multidisciplinary Management, and Outcome - A Case Report
OthersPage Navigation
Abstract
Lipoma is a benign mesenchymal tumor composed of mature adipocytes and represents the most common soft tissue tumor encountered in clinical practice. Although frequently asymptomatic and slow growing, lipomas may occasionally present diagnostic challenges when they occur in atypical locations, exhibit rapid growth, or cause compressive symptoms. Pediatric lipomas are relatively uncommon compared to adult cases and require careful evaluation to differentiate them from other benign and malignant soft tissue tumors.
We report a case of a subcutaneous lipoma in a pediatric patient presenting with a progressively enlarging, painless limb swelling. This case underscores the importance of thorough clinical examination, appropriate imaging for lesion characterization, histopathological confirmation, and a multidisciplinary approach to management to ensure optimal outcomes and avoid unnecessary interventions.
Introduction
Lipomas are benign tumors originating from adipose tissue and account for nearly half of all soft tissue tumors [1]. They are typically encapsulated, well circumscribed, and composed of mature fat cells without cellular atypia. Lipomas can occur anywhere in the body but are most commonly found in the subcutaneous tissues of the trunk, neck, shoulders, and proximal extremities.
While lipomas predominantly affect adults between the fourth and sixth decades of life, they may occasionally present in children and adolescents. Pediatric lipomas constitute a small proportion of soft tissue tumors and pose unique diagnostic considerations due to the broader differential diagnosis in this age group, including lipoblastoma, fibromatosis, vascular malformations, and soft tissue sarcomas [2].
Most lipomas are clinically benign and require no intervention unless symptomatic. However, lesions that increase in size, cause discomfort, restrict movement, or raise cosmetic or diagnostic concerns warrant further evaluation. Imaging modalities such as ultrasonography and magnetic resonance imaging (MRI) play a pivotal role in lesion characterization and surgical planning.
Case Report
Patient History
A 9-year-old female child was brought to the pediatric outpatient department with a complaint of a painless swelling over the posterior aspect of the left upper arm. The swelling was first noticed approximately six months prior and had gradually increased in size over time. There was no associated pain, redness, warmth, or history of trauma.

The caregivers denied any history of fever, weight loss, night sweats, or reduced appetite. There was no limitation of limb movement or interference with daily activities. The child had no significant past medical history and was not on long-term medication. Family history was unremarkable, with no known hereditary or connective tissue disorders.
Clinical Examination
On physical examination, the child was afebrile and hemodynamically stable. General examination revealed no pallor, lymphadenopathy, or signs of systemic illness.
Local examination of the left upper arm revealed a well-defined, soft, non-tender, and mobile mass measuring approximately 4 × 3 cm in the subcutaneous plane. The swelling had a smooth surface, was not adherent to the overlying skin or underlying muscle, and showed no signs of inflammation. The overlying skin appeared normal, with no discoloration or ulceration.

Neurovascular examination of the affected limb was normal, and there was full range of motion at the shoulder and elbow joints. Examination of other systems did not reveal any abnormalities.
Clinical Evaluation
Initial Differential Diagnosis
Based on the clinical presentation, the following differential diagnoses were considered:
- Lipoma
- Lipoblastoma
- Epidermoid cyst
- Benign fibrous tumor
- Soft tissue sarcoma
Given the slow growth, soft consistency, mobility, and absence of systemic symptoms, a benign soft tissue lesion was suspected. However, imaging was planned to further characterize the lesion and exclude malignancy.
Investigations
Radiological Evaluation
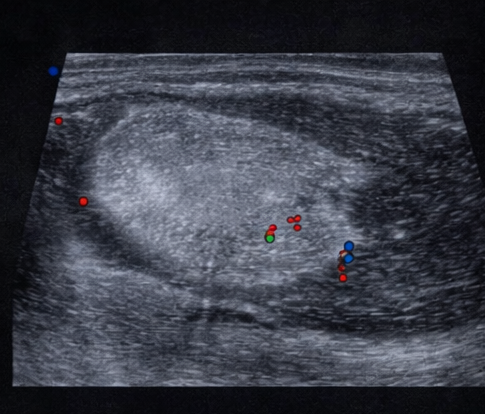
Ultrasound examination of the swelling revealed a well-circumscribed, homogenous, hyperechoic lesion located in the subcutaneous tissue. The lesion showed no internal calcification or cystic components and minimal internal vascularity on Doppler evaluation, favoring a benign fatty lesion.
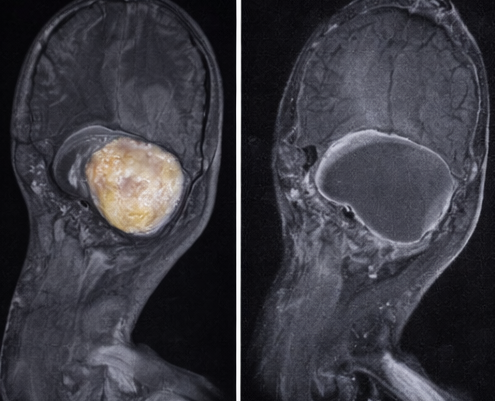
Magnetic resonance imaging (MRI) of the left upper arm was performed for further evaluation. MRI demonstrated a well-encapsulated lesion that was hyperintense on T1-weighted and T2-weighted images, with complete signal suppression on fat-suppressed sequences. There was no evidence of internal septal thickening, nodularity, hemorrhage, or invasion into adjacent muscular structures. These findings were highly suggestive of a benign lipomatous tumor.
Diagnosis
Based on the clinical features and imaging characteristics, a provisional diagnosis of subcutaneous lipoma was made. Surgical excision was planned both for definitive diagnosis and to alleviate parental concern.
Management and Outcome
Multidisciplinary Approach
The case was managed through a multidisciplinary team involving pediatric surgery, radiology, anesthesia, and pathology. Detailed counseling was provided to the caregivers regarding the benign nature of the lesion, the need for surgical excision, and the low risk of recurrence.
Therapeutic Management
The child underwent complete surgical excision of the mass under general anesthesia. Intraoperatively, a well-encapsulated, yellowish, lobulated fatty mass was identified in the subcutaneous plane and excised in toto without complications. There was no involvement of underlying muscle or neurovascular structures.
The excised specimen was sent for histopathological examination.

Histopathological Findings
Microscopic examination revealed mature adipocytes arranged in lobules separated by thin fibrous septae. There was no evidence of cellular atypia, lipoblasts, necrosis, or mitotic activity. These findings confirmed the diagnosis of a benign lipoma.
Follow-Up
The postoperative period was uneventful, and the child was discharged on the second postoperative day. At follow-up visits conducted at one month, three months, and six months, the patient remained asymptomatic with no evidence of recurrence. The surgical scar healed well, and the cosmetic outcome was satisfactory.

Discussion
Lipomas are benign adipocytic tumors with an excellent prognosis following complete excision. In pediatric patients, differentiation from lipoblastoma is particularly important, as lipoblastomas are more common in younger children and may show infiltrative growth patterns [3].
MRI is the imaging modality of choice for evaluating soft tissue tumors due to its superior soft tissue contrast and ability to delineate lesion extent. Typical lipomas demonstrate uniform fat signal intensity without suspicious features such as thick septae, nodularity, or enhancement, which may raise concern for liposarcoma [4].
Surgical excision is curative in the majority of cases and is indicated for symptomatic lesions, diagnostic uncertainty, or cosmetic reasons. Recurrence is rare and usually related to incomplete excision.
Conclusion
Lipoma should be considered in the differential diagnosis of painless, slowly enlarging soft tissue masses in pediatric patients. A structured diagnostic approach incorporating careful clinical evaluation, appropriate imaging, and histopathological confirmation is essential for accurate diagnosis and management. Multidisciplinary coordination and caregiver counseling play a key role in ensuring favorable outcomes and preventing unnecessary anxiety or interventions.
References
- Weiss SW, Goldblum JR. Enzinger and Weiss’s Soft Tissue Tumors. 6th ed. Elsevier; 2014.
- Kransdorf MJ. Benign soft-tissue tumors in a large referral population: distribution of specific diagnoses by age, sex, and location. AJR Am J Roentgenol. 1995;164(2):395–402.
- Chung EB, Enzinger FM. Benign lipoblastic tumors. Cancer. 1973;32(2):482–492.
- Bancroft LW, Kransdorf MJ. Imaging of soft tissue tumors. Radiol Clin North Am. 2011;49(6):1219–1234.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Researchers find distinct cell receptors with the potential for new treatments.
2.
Breast cancer patients' arms swell less after an effective lymph node transfer.
3.
Telehealth in the pandemic era resulted in fewer therapy interruptions.
4.
Too Many Chest CTs for Incidental Lung Nodules?
5.
Global warming could be driving up women's cancer risk, find researchers
1.
The New Frontier of Cancer Survivorship: Navigating the Long-Term Effects of Immunotherapy and Targeted Therapies
2.
Deterministic Reprogramming of Neutrophils within Tumors: A New Frontier in Cancer Research
3.
Neuroendocrine Tumors: Case Study on Diagnosis, Treatment Strategies & Patient Management
4.
Ticagrelor Monotherapy vs. Ticagrelor + Aspirin in ACS Post-PCI: ULTIMATE-DAPT Trial
5.
Transfusing the Future: Exploring the Possibilities of Blood Transfusions
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Current Scenario of Blood Cancer- A Conclusion on Genomic Testing & Advancement in Diagnosis and Treatment
2.
Navigating the Brain Barrier: The CNS Challenge in ALK+ NSCLC
3.
Thromboprophylaxis In Medical Settings
4.
Treatment Paradigm for Patients with R/R Adult B-cell ALL- Expert Discussions
5.
Current Scenario of Blood Cancer- Genomic Testing & Advancement in Diagnosis and Treatment

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge