Scoliosis: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes - A Case Report
OthersPage Navigation
Abstract
Scoliosis is a three-dimensional deformity of the spine characterized by lateral curvature and vertebral rotation, most commonly presenting during adolescence but also observed in adults due to degenerative changes. The condition may be idiopathic or secondary to neuromuscular, congenital, or syndromic causes. Clinical manifestations range from asymptomatic spinal asymmetry to back pain, postural imbalance, cosmetic concerns, and, in severe cases, cardiopulmonary compromise. Early identification and appropriate intervention are critical to prevent curve progression and long-term morbidity. We report a case of adolescent idiopathic scoliosis in a teenage female presenting with progressive spinal deformity and intermittent back pain. This case highlights clinical presentation, diagnostic evaluation including radiographic assessment, conservative management with bracing and physiotherapy, and short-term outcomes. The report emphasizes the importance of early screening, curve monitoring, individualized treatment planning, and patient education to optimize functional and psychosocial outcomes.
Introduction
Scoliosis is defined as a lateral spinal curvature with a Cobb angle ≥10° on standing radiographs, accompanied by vertebral rotation. Adolescent idiopathic scoliosis (AIS) accounts for approximately 80% of cases, typically presenting between 10 and 18 years of age, with a higher prevalence and risk of progression in females. The etiology of idiopathic scoliosis remains multifactorial, involving genetic predisposition, growth-related factors, and neuromuscular imbalance. Common curve patterns include thoracic, thoracolumbar, and lumbar deformities. Potential complications include progressive deformity, chronic back pain, reduced pulmonary function in severe thoracic curves, and psychosocial distress related to body image. Early diagnosis and timely intervention during periods of rapid growth are essential to prevent curve progression and reduce the need for surgical correction.
Case Report
Patient History
A 14-year-old female presented to the orthopedic outpatient clinic with a 6-month history of progressive asymmetry of the shoulders and mild, intermittent mid-back pain, aggravated by prolonged sitting and school activities. The deformity was first noticed by her parents during routine observation. There was no history of trauma, neurological symptoms, respiratory complaints, or prior spinal disorders. The patient had attained menarche 6 months earlier, suggesting ongoing growth potential. There was no family history of scoliosis or connective tissue disorders.
Clinical Examination
On inspection, the patient demonstrated right shoulder elevation, asymmetry of the waistline, and prominence of the right thoracic rib hump on forward bending (Adam’s forward bend test).

Postural imbalance was noted without pelvic obliquity. Neurological examination revealed normal motor strength, sensation, and deep tendon reflexes in all limbs. There were no cutaneous stigmata suggestive of underlying spinal dysraphism. Gait was normal, and no limb-length discrepancy was identified.
Clinical Evaluation
Differential Diagnosis
• Adolescent idiopathic scoliosis
• Postural scoliosis
• Congenital vertebral anomalies
• Neuromuscular scoliosis
• Leg length discrepancy–related spinal asymmetry
Investigations
Standing posteroanterior and lateral radiographs of the whole spine revealed a right thoracic curve with a Cobb angle of 32° (T5–T11) and mild vertebral rotation.
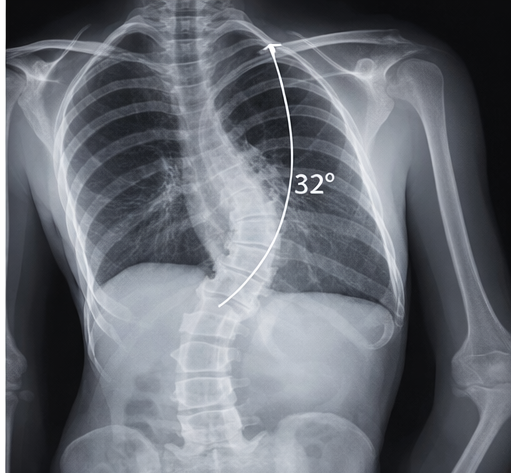
Risser sign was grade 1, indicating significant remaining growth potential and risk of progression. No congenital vertebral anomalies were identified. Magnetic resonance imaging (MRI) was not indicated due to the absence of neurological signs or atypical curve patterns. Baseline pulmonary function tests were within normal limits.
Management and Outcome
Management Strategy
Given the moderate curve magnitude and remaining skeletal growth, conservative management with thoracolumbosacral orthosis (TLSO) bracing was initiated, to be worn for 18–20 hours per day.

A structured physiotherapy program focusing on posture correction, core strengthening, and scoliosis-specific exercises (Schroth-based therapy) was prescribed. The patient and family were counseled regarding brace compliance, potential psychosocial challenges, and the importance of regular follow-up to monitor curve progression.

Analgesics (paracetamol) were advised on an as-needed basis for pain control.

Follow-Up and Outcome
At 6-month follow-up, the patient demonstrated good brace compliance, with repeat radiographs showing curve stabilization (Cobb angle reduced to 24° in-brace). The patient reported improvement in back discomfort and posture awareness. At 12-month follow-up, no significant curve progression was observed, and functional status remained preserved. The patient continued physiotherapy and brace use until nearing skeletal maturity. Ongoing monitoring was advised until growth completion to assess the need for escalation of care.
Discussion
Adolescent idiopathic scoliosis is the most common form of spinal deformity in children and adolescents. Curve progression is influenced by skeletal immaturity, female sex, and larger initial Cobb angles. Screening using physical examination and selective radiographic evaluation facilitates early detection. Bracing is the mainstay of treatment for moderate curves (25°–40°) in skeletally immature patients and has been shown to reduce the risk of progression to surgical thresholds. Physiotherapy complements bracing by improving posture, muscular balance, and patient engagement, though it does not replace brace therapy in preventing progression.
Surgical intervention is typically reserved for progressive curves exceeding 45°–50° or those associated with functional compromise. Psychosocial support is integral to management, as adolescents may experience body image concerns and reduced treatment adherence. Multidisciplinary care involving orthopedists, physiotherapists, and counselors improves long-term adherence and outcomes.
Conclusion
Scoliosis is a prevalent spinal deformity with a well-recognized potential for progression during periods of rapid growth, particularly in children and adolescents, and if left untreated, it may lead to functional limitations, chronic back pain, postural imbalance, cosmetic concerns, and significant psychosocial distress. Progressive spinal curvature can adversely affect physical function, participation in daily activities, and overall health-related quality of life, with severe deformities potentially resulting in restrictive pulmonary impairment and long-term musculoskeletal complications. Early clinical recognition through routine screening and careful physical examination, followed by appropriate radiographic assessment using standardized measurements such as the Cobb angle, is essential for accurate diagnosis and staging of disease severity. Risk stratification based on growth potential, skeletal maturity, curve magnitude, and pattern is critical to guide timely and individualized intervention strategies.
Conservative management, including evidence-based brace therapy and scoliosis-specific physiotherapy programs, can effectively stabilize moderate curves in skeletally immature patients, reduce the risk of curve progression, and delay or prevent the need for surgical intervention. Treatment success is strongly influenced by early initiation, adherence to bracing protocols, and active patient engagement in rehabilitation programs. Long-term follow-up through skeletal maturity is necessary to monitor curve progression, treatment response, and potential complications, allowing timely escalation of care when indicated. In addition to physical management, comprehensive scoliosis care should incorporate structured patient education, family involvement, and psychosocial support to address body image concerns, treatment adherence challenges, and emotional well-being, ultimately improving functional outcomes, treatment satisfaction, and long-term quality of life.
References
- Weinstein SL, Dolan LA, Cheng JCY, Danielsson A, Morcuende JA. Adolescent idiopathic scoliosis. Lancet. 2008;371(9623):1527–1537.
- Negrini S, Donzelli S, Aulisa AG, et al. 2016 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. 2018;13:3.
- Dolan LA, Wright JG, Weinstein SL. Effects of bracing in adolescents with idiopathic scoliosis. N Engl J Med. 2013;369:1512–1521.
- Hresko MT. Clinical practice. Idiopathic scoliosis in adolescents. N Engl J Med. 2013;368:834–841.
- Negrini A, Negrini MG, Donzelli S, et al. Scoliosis-specific exercises can reduce curve progression in adolescents with idiopathic scoliosis. Physiother Theory Pract. 2019;35(5):443–451.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Sub-Q Ketamine is Safe and Very Effective for Severe Depression.
2.
Study indicates that exercise can help colon cancer survivors live as long as matched individuals
3.
Contradictory Results Are Found in Two Pembrolizumab Trials for Head and Neck Cancer.
4.
Can Concurrent Boost Safely Shorten Breast Cancer Radiation?
5.
Positive Trials; Malignancies Increasing in Younger Adults; Andre Braugher's Cancer Dx.
1.
Trends in Incidence, Care, and Surgery for Medullary Thyroid Cancer: A Review
2.
Antibody-Drug Conjugates in Oncology: Breakthroughs, Clinical Updates, and Pipeline Innovation
3.
Navigating the Stages of Thyroid Cancer: A Guide for Patients
4.
Polycythemia Vera: A Historical Perspective and Contemporary Management
5.
Glofitamab: A Breakthrough Therapy for Relapsed/Refractory Mantle Cell Lymphoma
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Pazopanib: A Game-Changer in Managing Advanced Renal Cell Carcinoma - Part IV
2.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VIII
3.
Evolving Space of First-Line Treatment for Urothelial Carcinoma- Case Discussion
4.
Key Takeaways from The CROWN Trial For ALK + NSCLC Patients with CNS Diseases
5.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part I

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge