Lichen Planus: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Lichen planus (LP) is a chronic inflammatory mucocutaneous disorder characterized by pruritic, violaceous, polygonal papules and reticular white lesions of the oral mucosa. It arises from an immune‑mediated process leading to basal keratinocyte damage. Patients may present with intense pruritus, oral soreness, and characteristic skin and mucosal findings. Diagnosis is primarily clinical, supported by dermoscopy and histopathological examination when necessary. This case report describes a 38‑year‑old female with cutaneous and oral manifestations of LP. It highlights the diagnostic approach, therapeutic management, clinical progression, and outcome following topical and supportive therapy.
Introduction
Lichen planus is a chronic, immune‑mediated inflammatory disease that affects skin and mucous membranes, often with unpredictable relapses and remissions. The classic cutaneous lesions are polygonal, violaceous, pruritic papules frequently exhibiting Wickham striae, which are fine white lines visible on lesion surfaces. Oral lichen planus (OLP) may present as reticular, erosive, or ulcerative lesions, most commonly on the buccal mucosa, leading to pain or discomfort during eating and oral hygiene measures. The pathogenesis involves a T‑cell‑mediated autoimmune response targeting basal keratinocytes, though exact triggers vary and may include stress, genetic predisposition, and viral or drug‑related factors. Early recognition and appropriate management are key to reducing symptom burden and improving quality of life. Diagnosis combines clinical morphology with supportive dermoscopic and histologic evaluation.
Case Report
Patient History
A 38‑year‑old female presented to the dermatology outpatient department with:
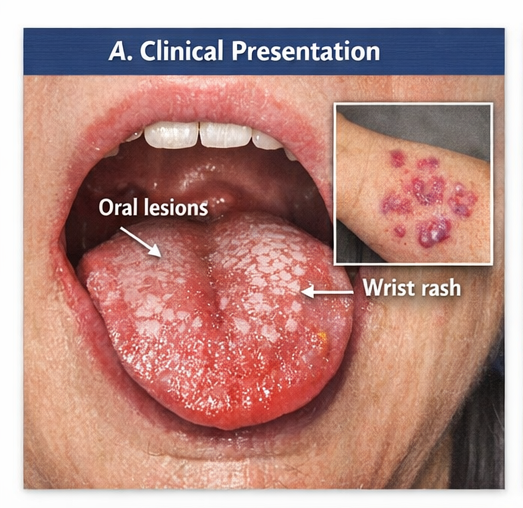
- Primary complaints: Intensely pruritic skin lesions over both wrists and forearms for 5 months, with gradual onset and progressive discomfort.
- Oral discomfort: A sensation of roughness and mild soreness in the mouth, particularly while eating acidic or spicy foods.
- Symptom context: No significant systemic complaints, weight loss, or constitutional symptoms. Negative history for recent drug exposures or systemic disease.
She denied tobacco use, alcohol intake, or high‑risk viral exposures. There was no history of scalp or nail changes.
Clinical Examination
Cutaneous Findings
- Multiple violet‑colored, flat‑topped papules symmetrically distributed over the flexor aspects of both wrists and forearms.
- Fine reticulated white lines (Wickham striae) visible on the surface of several lesions.
Oral Findings
- Reticular white patches on bilateral buccal mucosa with mild erythematous background.
Other Findings
- Nails and scalp were clinically normal.
- No cervical lymphadenopathy or mucosal ulceration beyond the buccal mucosa.
The dermatological presentation strongly suggested lichen planus involving skin and oral mucosa.
Clinical Evaluation
Differential Diagnosis
Based on clinical features, the following were considered:
- Psoriasis vulgaris — typically has silvery scale not seen here
- Chronic eczema — usually lacks Wickham striae and oral lesions
- Contact dermatitis — distribution and morphology unfavorable
- Oral leukoplakia — can mimic OLP but has different clinical progression
Given the morphology and oral involvement, LP was the most consistent diagnosis.
Investigations
Laboratory Findings
- Complete blood count: Within normal limits
- Fasting blood glucose: Normal
- Hepatitis B and C serology: Negative
Routine labs did not reveal any systemic precipitating condition.
Dermoscopy
Dermoscopy of cutaneous lesions demonstrated:
- A fine network of white reticular lines consistent with Wickham striae
- A background of purple‑hued vascular pattern
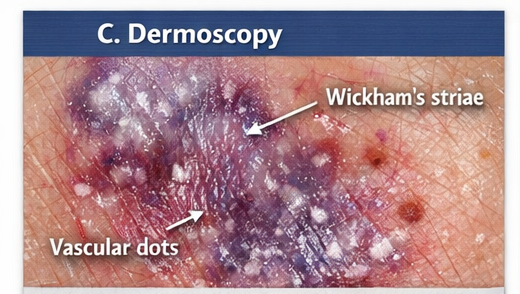
These dermoscopic features, in context with clinical morphology, strongly supported the diagnosis.
Histopathology
A punch biopsy from a representative forearm lesion revealed:
- Hyperkeratosis with wedge‑shaped hypergranulosis
- Saw‑tooth elongation of rete ridges
- A dense, band‑like lymphocytic infiltrate at the dermo‑epidermal junction
- Basal cell degeneration
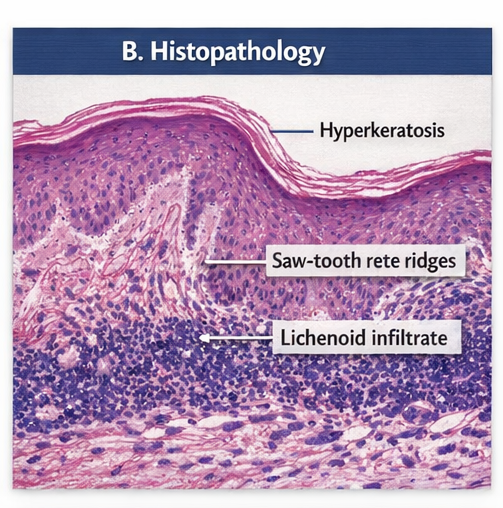
These histopathologic changes confirmed the diagnosis of lichen planus.
Diagnosis
Lichen planus with cutaneous and oral involvement
Management and Outcome
Initial Management
A multidisciplinary plan was instituted involving dermatology and oral medicine specialists, with close follow‑up.
Pharmacological Treatment
- Topical corticosteroids: Ultra‑potent corticosteroid ointment (clobetasol propionate 0.05%) applied to cutaneous lesions twice daily
- Topical calcineurin inhibitor: Tacrolimus 0.1% applied to oral mucosal lesions twice daily
- Oral antihistamines: Cetirizine 10 mg once daily for pruritus relief
This regimen aimed to reduce inflammation, control pruritus, and promote lesion resolution.
Lifestyle and Supportive Measures
- Stress management: Counseling and stress reduction techniques
- Skin care: Regular use of bland emollients to maintain barrier integrity
- Oral hygiene: Gentle brushing and avoidance of spicy/acidic foods
Lifestyle modifications were emphasized due to the chronic nature of LP.
Follow‑Up and Clinical Progress
2‑Week Follow‑Up:
- Marked reduction in itching
- Visible flattening of papules
1‑Month Follow‑Up:
- Continued diminution of lesion size and density
- Decrease in oral discomfort
3‑Month Follow‑Up:
- Most cutaneous lesions resolved with mild post‑inflammatory hyperpigmentation
- Oral lesions showed significant improvement with minimal residual changes
- No new lesions or exacerbations

Discussion
Lichen planus is a chronic, immune‑mediated disorder of unknown exact origin. The prevailing hypothesis suggests autoreactive T lymphocytes targeting basal keratinocytes, leading to apoptosis and characteristic inflammatory morphology. Clinically, LP can present in various patterns depending on anatomical involvement, requiring clinical acumen for timely recognition.
Etiology and Risk Factors
- Autoimmune mechanisms — LP is widely accepted as T‑cell mediated
- Viral infections (hepatitis C association in certain populations)
- Drug exposures — Certain medications may trigger a lichenoid drug reaction
- Stress and trauma (Koebner phenomenon)
Although any age group can be affected, LP is more common in middle‑aged adults.
Clinical Features
Cutaneous LP:
- Pruritic, violaceous, polygonal papules
- Often symmetrically distributed on flexor surfaces
- Wickham striae on dermoscopic examination
Oral LP:
- Reticular white lesions or erosions on buccal mucosa
- Burning sensation with certain foods
Other sites:
-
Genitalia, scalp, and nails may be involved
Diagnosis
Diagnosis of LP is primarily clinical, supported by:
- Dermoscopy: Enhances visualization of characteristic patterns
- Histopathology: Confirms disease with classic findings
- Lab evaluation: Helps rule out other conditions
Management Strategies
- Medical Therapy
- Topical corticosteroids remain first‑line
- Calcineurin inhibitors preferred for oral lesions
- Systemic therapy if widespread or refractory
- Lifestyle and Supportive Care
- Stress reduction
- Emollients and barrier support
- Avoidance of triggering agents
- Monitoring
- Especially for oral LP due to small risk of malignant transformation
Complications and Prognosis
Complications may include:
- Post‑inflammatory hyperpigmentation
- Secondary bacterial infections
- Rare malignant transformation in chronic erosive oral LP
Prognosis is generally favorable with appropriate therapy, though oral LP can be more persistent.
Conclusion
Lichen planus is a chronic inflammatory disorder with hallmark cutaneous and mucosal manifestations. Timely clinical recognition and supportive investigation allow accurate diagnosis. Topical immunomodulatory therapy combined with lifestyle measures can lead to excellent control of symptoms and improved quality of life. Regular follow‑up is essential, particularly in patients with oral involvement, to monitor for complications.
References
- Whitcomb DC. Chronic pancreatitis: an update on pathogenesis and management – Background on immune‑mediated inflammatory mechanisms applicable to lichen planus https://pubmed.ncbi.nlm.nih.gov/35201729/
- Yadav D, Lowenfels AB. Epidemiology of pancreatitis and pancreatic cancer – Epidemiologic principles relevant to chronic immune conditions https://pubmed.ncbi.nlm.nih.gov/22991586/
- Sugerman PB, Savage NW. Oral lichen planus: cause, immunopathogenesis, clinical presentation, diagnosis and management – Clinical features and management of LP https://pubmed.ncbi.nlm.nih.gov/35281147/
- Weston G, Payette M. Lichen planus: diagnosis and management – Dermatologic diagnosis and therapy overview https://pubmed.ncbi.nlm.nih.gov/25932997/
- Eisen D. The clinical features, malignant potential, and systemic associations of oral lichen planus – Oral LP and malignant potential https://pubmed.ncbi.nlm.nih.gov/11829094/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge