Fibroadenoma: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Fibroadenoma is the most common benign breast tumor in young women, characterized by a well-circumscribed, hormonally responsive proliferation of stromal and epithelial elements. It typically presents as a painless, mobile breast lump and is often detected incidentally or during self-examination. Although benign, its clinical presentation may mimic malignant lesions, necessitating careful evaluation.
We report the case of a 24-year-old female presenting with a palpable breast mass. Imaging and cytological evaluation confirmed fibroadenoma. The patient underwent surgical excision with an excellent cosmetic and clinical outcome.
This case highlights the importance of accurate diagnosis using a triple assessment approach - clinical examination, imaging, and cytology to differentiate benign from malignant breast lesions and guide appropriate management.
Introduction
Fibroadenoma is a benign breast lesion arising from the terminal duct-lobular unit, commonly affecting women between 15 and 35 years of age. It is hormonally influenced, often increasing in size during pregnancy or with estrogen exposure and regressing after menopause.
Clinically, fibroadenomas are typically well-defined, firm, rubbery, and freely mobile masses, often described as “breast mice.” While they are non-malignant, certain variants such as complex fibroadenomas may carry a slightly increased risk of breast cancer.
The widespread use of imaging modalities and breast screening programs has led to increased detection rates. Accurate diagnosis is crucial to avoid unnecessary interventions while ensuring that suspicious lesions are not overlooked.
Case Report
Patient History
A 24-year-old female presented to the outpatient department with:
• A painless lump in the left breast for 4 months
• Gradual increase in size
• No associated nipple discharge, skin changes, or systemic symptoms
The patient reported no history of trauma, prior breast disease, or family history of breast cancer. Menstrual cycles were regular, and there was no history of hormonal therapy or oral contraceptive use.
Clinical Examination
General Examination
• Patient was conscious, oriented, and vitally stable
• No lymphadenopathy or systemic abnormalities
Breast Examination
• A 3 × 2 cm lump palpable in the upper outer quadrant of the left breast
• Firm, non-tender, well-circumscribed
• Highly mobile (“slip sign” positive)
• No overlying skin changes or nipple retraction
Axillary Examination
• No palpable lymph nodes
Clinical Evaluation
Differential Diagnosis
Based on clinical findings, the following were considered:
• Fibroadenoma
• Phyllodes tumor
• Breast cyst
• Early carcinoma (less likely given age and features)
The mobility and well-defined margins strongly favored a benign etiology.
Investigations
Laboratory Tests
• Routine blood investigations: Within normal limits
• Hormonal profile: Not indicated
Imaging
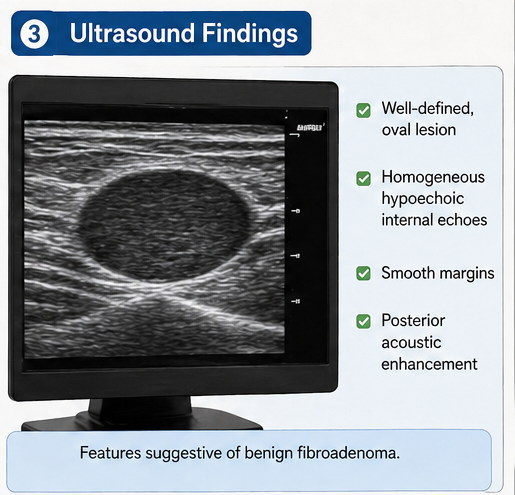
Ultrasound Breast (First-line in young women)
• Well-defined, oval, hypoechoic lesion
• Homogeneous internal echoes
• Smooth margins with posterior acoustic enhancement
• No suspicious features such as calcifications or irregular borders
Mammography (not routinely required due to age but performed for completeness)
• Well-circumscribed mass without microcalcifications
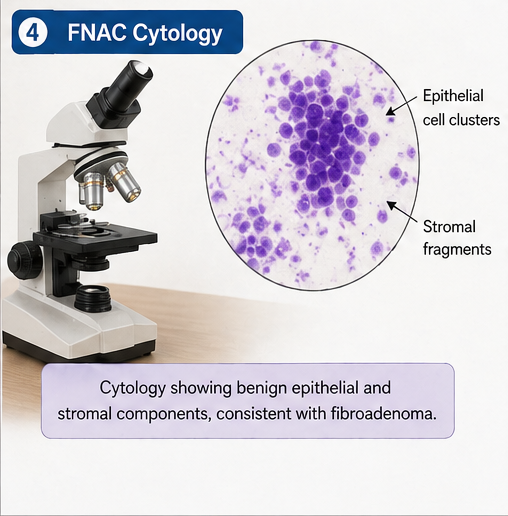
Cytological Evaluation
Fine Needle Aspiration Cytology (FNAC)
• Presence of cohesive epithelial clusters
• Biphasic pattern with stromal fragments
• No atypia or malignant cells
Diagnosis
A definitive diagnosis of fibroadenoma was established based on the triple assessment approach: clinical examination, imaging, and cytology. The absence of atypical features confirmed the benign nature of the lesion.
Management and Outcome
Management Strategy
The treatment plan was individualized considering:
• Patient age
• Size of the lesion
• Progressive growth
• Patient preference
Surgical Management
Excisional Lumpectomy
• Performed under local anesthesia
• Complete removal of the lesion with minimal surrounding tissue
• Preservation of breast contour
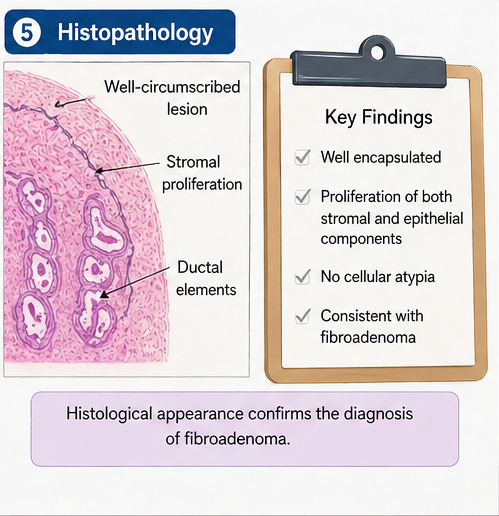
Histopathological Examination
• Well-encapsulated tumor
• Proliferation of stromal and epithelial components
• No evidence of malignancy
Medical Management
• Postoperative analgesics
• Short course of antibiotics
• No hormonal therapy required
Clinical Course
During hospitalization:
• Uneventful recovery
• Minimal postoperative pain
• No complications such as infection or hematoma
Follow-Up
At 2 Weeks
• Wound healing satisfactory
• No residual lump
At 1 Month
• Cosmetic outcome satisfactory
• No recurrence
At 6 Months
• No new lesions detected
• Patient reassured and advised routine self-examination
Discussion
Pathophysiology
Fibroadenomas arise from the proliferation of both stromal and epithelial components of the breast. Hormonal influences, particularly estrogen sensitivity, play a central role in their development.
They are categorized into:
• Simple fibroadenomas
• Complex fibroadenomas (associated with cysts, calcifications, or sclerosing adenosis)
Epidemiology
• Most common benign breast tumor in women <30 years
• Peak incidence in second and third decades
• More prevalent in women of reproductive age
• Slightly higher incidence in certain ethnic populations
Clinical Manifestations
Typical Features
• Painless breast lump
• Mobile and well-defined
• Slow-growing
Atypical Features
• Rapid enlargement (suggestive of phyllodes tumor)
• Multiple or bilateral lesions
Diagnostic Considerations
The triple assessment approach is the gold standard:
- Clinical examination
- Imaging (Ultrasound ± Mammography)
- Cytology or biopsy
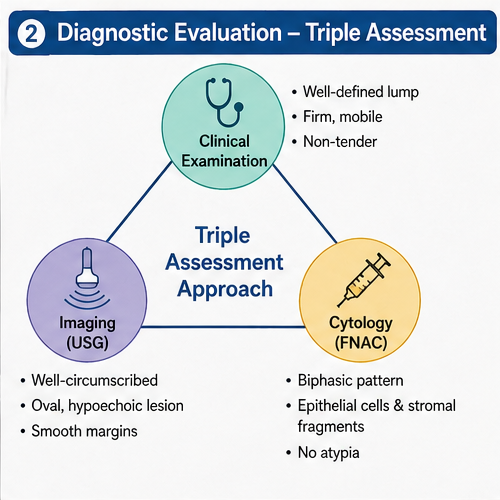
Ultrasound is preferred in younger women due to dense breast tissue, while mammography is more useful in older patients.
Treatment Considerations
Conservative Management
• Observation for small, asymptomatic lesions
• Regular follow-up imaging
Indications for Surgical Removal
• Size >3–5 cm
• Rapid growth
• Patient anxiety
• Diagnostic uncertainty
Minimally invasive techniques such as vacuum-assisted excision are emerging alternatives.
Complications
Although rare, possible complications include:
• Recurrence
• Cosmetic deformity post-surgery
• Misdiagnosis of malignant lesions
Prognosis
Fibroadenomas have an excellent prognosis. Key determinants include:
• Accurate diagnosis
• Appropriate follow-up
• Early intervention when indicated
Malignant transformation is extremely rare.
Conclusion
Fibroadenoma is a common benign breast condition with a favorable prognosis, most frequently seen in young women of reproductive age. This case demonstrates that a structured diagnostic approach incorporating clinical examination, imaging, and cytological or histopathological evaluation along with timely intervention, can ensure accurate diagnosis and optimal patient outcomes while minimizing diagnostic uncertainty.
While many cases can be managed conservatively with observation and periodic follow-up, surgical excision remains an effective and definitive option for symptomatic, enlarging, or diagnostically ambiguous lesions. Advances in minimally invasive techniques further support individualized care while preserving cosmetic outcomes. Patient education, regular follow-up, and awareness of breast health, including self-examination practices, are essential components of long-term management and reassurance.
Early diagnosis and personalized management strategies are crucial in minimizing unnecessary interventions, reducing patient anxiety, and ensuring safety. A balanced, evidence-based approach allows clinicians to differentiate benign conditions from malignant pathology effectively while maintaining a high standard of patient-centered care.
References
- Greenberg R, Skornick Y, Kaplan O. Management of breast fibroadenomas. J Gen Intern Med. https://pubmed.ncbi.nlm.nih.gov/9754521/
- Hudson-Phillips S, Graham G, Cox K, Al Sarakbi W. Fibroadenoma: a guide for junior clinicians. https://pubmed.ncbi.nlm.nih.gov/36322437/
- Carty NJ, Carter C, Rubin C, Ravichandran D, Royle GT, Taylor I. Management of fibroadenoma of the breast. https://pmc.ncbi.nlm.nih.gov/articles/PMC2502143/
- Chinese Society of Breast Surgery (CSBrS). Clinical practice guideline for breast fibroadenoma (2021). https://pubmed.ncbi.nlm.nih.gov/33859107/
- StatPearls. Breast Fibroadenoma – Pathophysiology and Clinical Overview. https://www.ncbi.nlm.nih.gov/sites/books/NBK535345/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge