Carcinoma of Tongue: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Carcinoma of the tongue is a common malignancy of the oral cavity, predominantly arising as squamous cell carcinoma. It is strongly associated with risk factors such as tobacco use, alcohol consumption, and poor oral hygiene. Patients typically present with non-healing ulcers, pain, dysphagia, and difficulty in speech. Early diagnosis is critical, as delayed presentation is often associated with advanced disease and poorer prognosis. Diagnostic evaluation includes clinical examination, imaging modalities, and histopathological confirmation through biopsy. Management involves a multidisciplinary approach including surgery, radiotherapy, and chemotherapy. This report describes a case of carcinoma of the lateral border of the tongue in a middle-aged patient, highlighting clinical features, diagnostic workup, and successful management.
Introduction
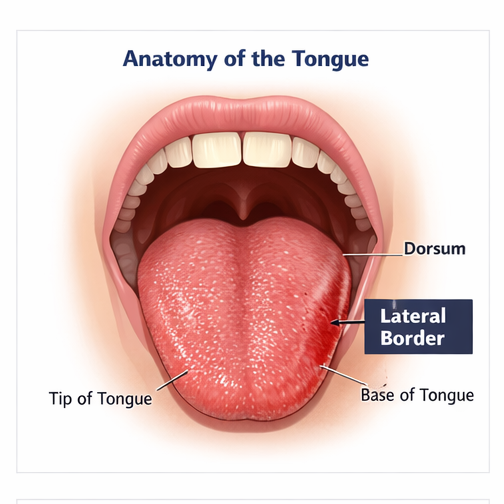
Carcinoma of the tongue is one of the most common malignancies of the oral cavity, accounting for a significant proportion of head and neck cancers. The majority of these tumors are oral squamous cell carcinomas, typically arising from the lateral borders of the tongue.
The pathogenesis involves chronic exposure to carcinogens such as tobacco (smoked and smokeless forms), alcohol, and in some cases, viral infections such as human papillomavirus (HPV). These factors lead to epithelial dysplasia, which may progress to invasive carcinoma over time.
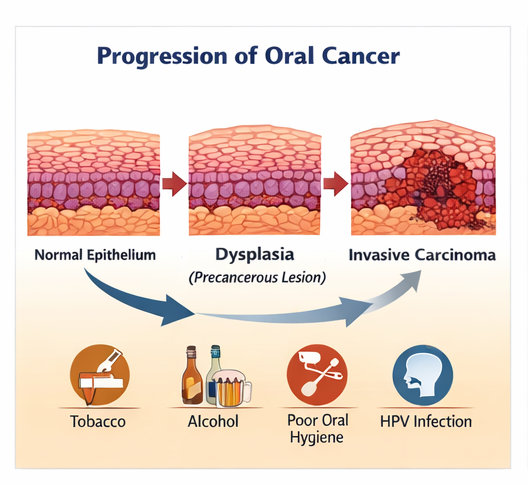
Risk factors include:
- Tobacco chewing and smoking
- Chronic alcohol consumption
- Poor oral hygiene
- Nutritional deficiencies
- Chronic irritation (sharp teeth, ill-fitting dentures)
Clinically, patients may present with a persistent ulcer, indurated lesion, pain, bleeding, or restricted tongue movement. Advanced cases may show cervical lymph node involvement due to early lymphatic spread.
Early diagnosis and prompt management are crucial, as prognosis is highly dependent on the stage at presentation. This case report highlights the clinical course of a patient with carcinoma of the tongue and emphasizes the importance of early detection and multidisciplinary care.
Case Report
Patient History
A 58-year-old male presented to the otorhinolaryngology outpatient department with complaints of a non-healing ulcer on the right side of the tongue for three months.
The patient reported:
- Persistent pain in the oral cavity
- Difficulty in swallowing (dysphagia)
- Occasional bleeding from the lesion
- Progressive difficulty in speech
There was a significant history of tobacco chewing for over 20 years and occasional alcohol consumption. The patient also reported poor oral hygiene. There was no history of prior malignancy or radiation exposure.
Clinical Examination
On general examination, the patient was moderately built with stable vital signs.
Local examination revealed:
- An ulceroproliferative lesion measuring approximately 3 × 2 cm on the right lateral border of the tongue
- Irregular margins with induration
- Tenderness on palpation
- Restricted mobility of the tongue
Neck examination revealed:
- A palpable, firm, non-tender lymph node in the right cervical region (Level II)
Oral cavity examination showed no other lesions.
Clinical Evaluation
Differential Diagnosis
Based on the clinical findings, the following differential diagnoses were considered:
- Squamous cell carcinoma of the tongue
- Traumatic ulcer
- Tuberculous ulcer
- Leukoplakia with malignant transformation
Further investigations were performed to establish a definitive diagnosis.
Investigations
Biopsy and Histopathology
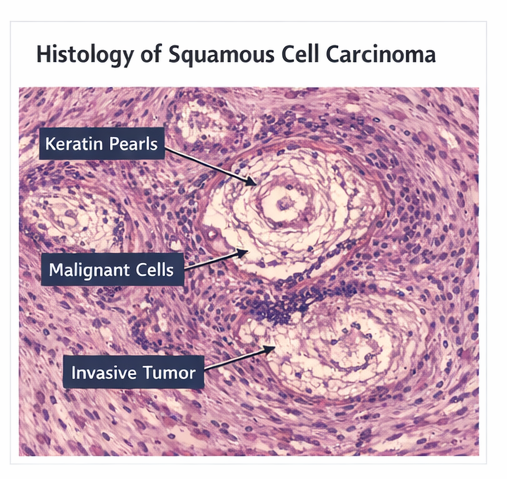
An incisional biopsy of the lesion was performed. Histopathological examination revealed:
- Invasive nests and cords of malignant squamous epithelial cells
- Keratin pearl formation
- Cellular atypia and increased mitotic activity
These findings confirmed the diagnosis of well-differentiated squamous cell carcinoma.
Imaging Studies
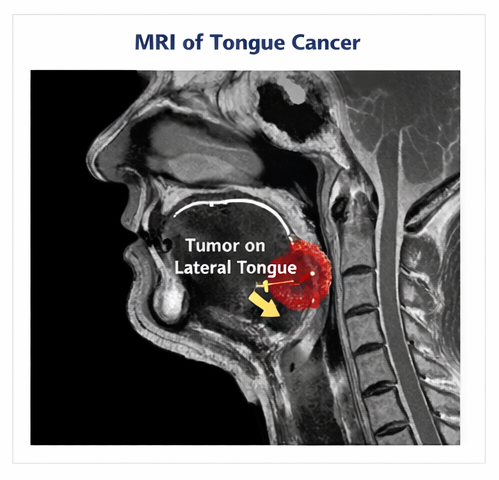
Magnetic Resonance Imaging (MRI):
MRI of the oral cavity showed:
- A lesion involving the right lateral border of the tongue
- Extension into intrinsic tongue muscles
- No involvement of the mandible
Computed Tomography (CT) Scan of Neck:
- Enlarged right cervical lymph node (Level II)
- No evidence of distant metastasis
Laboratory Investigations
- Complete blood count: within normal limits
- Liver and renal function tests: normal
- Viral markers (HIV, hepatitis): negative
Diagnosis
Based on clinical findings, imaging, and histopathological confirmation, the patient was diagnosed with:
Carcinoma of the tongue (right lateral border) – Stage III (T2N1M0)
Management and Outcome
Initial Management
A multidisciplinary tumor board discussion was conducted involving an oncologist, head and neck surgeon, and radiation specialist.
The patient was planned for:
- Surgical resection (partial glossectomy)
- Selective neck dissection (right side)
- Followed by adjuvant radiotherapy
Surgical Intervention
The patient underwent partial glossectomy with adequate margins along with right-sided neck dissection.
Intraoperative findings confirmed:
- Localized tumor with no mandibular invasion
- Involved cervical lymph node successfully excised
Postoperative Course
The postoperative period was uneventful. The patient was able to tolerate oral intake gradually and was referred for speech and swallowing rehabilitation.
Adjuvant Therapy
Histopathology of the resected specimen confirmed:
- Tumor-free margins
- One positive lymph node
Based on these findings, the patient received adjuvant radiotherapy to reduce the risk of recurrence.
Follow-Up and Outcome
The patient was followed up regularly over six months.
Clinical outcomes included:
- No evidence of local recurrence
- Improved speech and swallowing function
- Good wound healing
The patient reported significant relief from symptoms and improved quality of life.
Regular follow-up with clinical examination and imaging was advised to monitor for recurrence.
Discussion
Carcinoma of the tongue is a significant public health concern, particularly in regions with high prevalence of tobacco use. It is characterized by aggressive behavior and early lymphatic spread.
The most common histological type is squamous cell carcinoma, arising from the mucosal epithelium. The lateral border of the tongue is the most frequently affected site due to prolonged exposure to carcinogens.
The progression from premalignant lesions such as leukoplakia to invasive carcinoma involves genetic mutations, dysplasia, and eventual invasion of underlying tissues.
Clinically, early-stage lesions may present as painless ulcers, often leading to delayed diagnosis. Advanced disease presents with pain, dysphagia, speech difficulty, and cervical lymphadenopathy.
Biopsy remains the gold standard for diagnosis, while imaging modalities such as MRI and CT scans help in staging and treatment planning.
Management depends on tumor stage:
- Early-stage disease: surgery or radiotherapy
- Advanced disease: combined modality treatment (surgery + radiotherapy ± chemotherapy)
Surgical resection with adequate margins remains the cornerstone of treatment. Neck dissection is essential in cases with nodal involvement.
Adjuvant radiotherapy improves local control and survival in patients with high-risk features such as nodal metastasis or positive margins.
Prognosis depends on:
- Tumor stage
- Lymph node involvement
- Depth of invasion
- Treatment adequacy
Early-stage disease has a favorable prognosis, whereas advanced disease carries a higher risk of recurrence and mortality.
Preventive strategies include tobacco cessation, alcohol moderation, and regular oral screening, especially in high-risk populations.
Conclusion
Carcinoma of the tongue is a potentially life-threatening malignancy that requires early diagnosis and prompt intervention.
Persistent oral ulcers, especially in high-risk individuals, should always be evaluated thoroughly with biopsy.
A multidisciplinary approach involving surgery, radiotherapy, and rehabilitation is essential for optimal outcomes.
With timely treatment and regular follow-up, favorable clinical outcomes and improved quality of life can be achieved, as demonstrated in this case.
References
- National Comprehensive Cancer Network (NCCN). Head and Neck Cancers Guidelines. https://pubmed.ncbi.nlm.nih.gov/32145116/
- Warnakulasuriya S. Global epidemiology of oral and oropharyngeal cancer. https://pubmed.ncbi.nlm.nih.gov/26318599/
- Siegel RL, et al. Cancer statistics. CA Cancer J Clin. https://pubmed.ncbi.nlm.nih.gov/31912902/
- Shah JP, Gil Z. Current concepts in management of oral cancer. https://pubmed.ncbi.nlm.nih.gov/20851920/
- Lydiatt WM, et al. AJCC Cancer Staging Manual. https://pubmed.ncbi.nlm.nih.gov/30151625/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Sub-Q Ketamine is Safe and Very Effective for Severe Depression.
2.
Study indicates that exercise can help colon cancer survivors live as long as matched individuals
3.
Contradictory Results Are Found in Two Pembrolizumab Trials for Head and Neck Cancer.
4.
Can Concurrent Boost Safely Shorten Breast Cancer Radiation?
5.
Positive Trials; Malignancies Increasing in Younger Adults; Andre Braugher's Cancer Dx.
1.
Trends in Incidence, Care, and Surgery for Medullary Thyroid Cancer: A Review
2.
Antibody-Drug Conjugates in Oncology: Breakthroughs, Clinical Updates, and Pipeline Innovation
3.
Navigating the Stages of Thyroid Cancer: A Guide for Patients
4.
Polycythemia Vera: A Historical Perspective and Contemporary Management
5.
Glofitamab: A Breakthrough Therapy for Relapsed/Refractory Mantle Cell Lymphoma
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Pazopanib: A Game-Changer in Managing Advanced Renal Cell Carcinoma - Part IV
2.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VIII
3.
Evolving Space of First-Line Treatment for Urothelial Carcinoma- Case Discussion
4.
Key Takeaways from The CROWN Trial For ALK + NSCLC Patients with CNS Diseases
5.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part I

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge