Vitiligo: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Vitiligo is a chronic acquired depigmenting disorder characterized by the selective destruction of melanocytes, resulting in well-demarcated hypopigmented or depigmented macules and patches on the skin. Although not life-threatening, vitiligo significantly impacts psychological well-being and quality of life. The condition is widely considered autoimmune in origin, with genetic, environmental, and oxidative stress factors contributing to its pathogenesis.
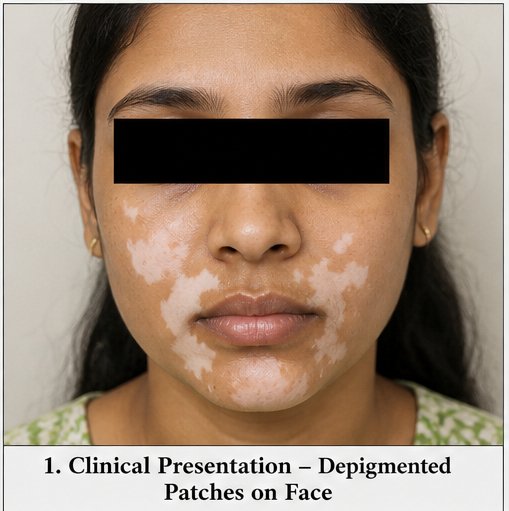
We report the case of a 28-year-old female presenting with progressive depigmented patches over the hands and face. Clinical examination and Wood’s lamp evaluation confirmed vitiligo. Laboratory findings suggested an associated autoimmune predisposition. The patient was managed with topical corticosteroids, calcineurin inhibitors, and narrowband ultraviolet B (NB-UVB) therapy, resulting in partial repigmentation and stabilization of disease progression.
This case highlights the importance of early diagnosis, comprehensive evaluation for associated autoimmune conditions, and a multimodal treatment approach in managing vitiligo effectively.
Introduction
Vitiligo is an acquired pigmentary disorder characterized by the loss of functional melanocytes from the epidermis, leading to depigmented skin lesions. It affects approximately 0.5–2% of the global population and can occur at any age, with peak onset in the second and third decades of life.
The condition is classified broadly into segmental and non-segmental types, with non-segmental vitiligo being the most common. The disease course is unpredictable, ranging from slow progression to rapid and widespread depigmentation.
The etiology of vitiligo is multifactorial, involving autoimmune destruction of melanocytes, genetic susceptibility, oxidative stress, and neural mechanisms. It is often associated with other autoimmune disorders such as thyroid disease, diabetes mellitus, and pernicious anemia.
Early diagnosis and intervention are crucial to limit disease progression and improve cosmetic outcomes. Despite advances in therapy, vitiligo remains a therapeutic challenge due to its chronic and relapsing nature.
Case Report
Patient History
A 28-year-old female presented to the dermatology outpatient department with:
- Progressive white patches over the face and hands for 8 months
- Mild itching occasionally at lesion sites
- No pain, scaling, or discharge
- Increasing cosmetic concern and psychological distress

There was no history of trauma, chemical exposure, or prior skin disease. The patient denied any history of similar lesions in childhood.
Medical history revealed hypothyroidism diagnosed 2 years prior, for which she was on regular medication. There was no history of diabetes or other chronic illnesses.
Family history was significant for autoimmune thyroid disease in her mother.
Clinical Examination
General Examination
- Patient conscious and oriented
- Vitals stable
- No pallor, icterus, or lymphadenopathy
Dermatological Examination
- Multiple well-defined depigmented macules and patches
- Distribution: perioral region, periocular area, dorsal hands, and fingers
- Lesions symmetrical in distribution
- No scaling or erythema
- Hair within lesions showed early depigmentation (leukotrichia)
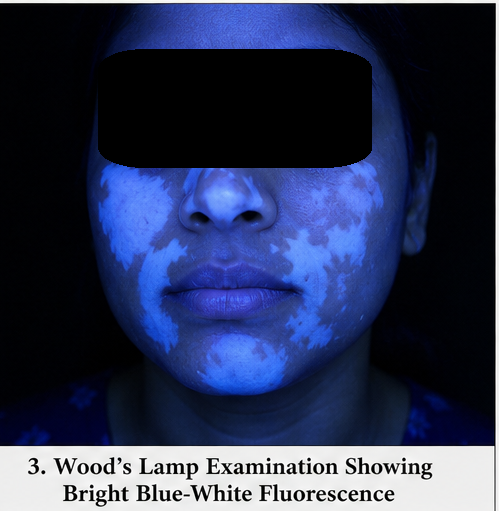
Wood’s Lamp Examination
- Lesions showed bright blue-white fluorescence, confirming depigmentation
Systemic Examination
- No significant abnormalities detected
Clinical Evaluation
Differential Diagnosis
Based on clinical findings, the following were considered:
- Vitiligo (most likely)
- Pityriasis alba
- Tinea versicolor
- Post-inflammatory hypopigmentation
- Chemical leukoderma
The absence of scaling, characteristic distribution, and Wood’s lamp findings strongly supported vitiligo.
Investigations
Laboratory Tests
- Complete blood count: Within normal limits
- Thyroid function tests: Elevated TSH (suggestive of suboptimal control)
- Anti-thyroid peroxidase (anti-TPO) antibodies: Positive
- Fasting blood glucose: Normal
- Vitamin B12 levels: Mildly reduced
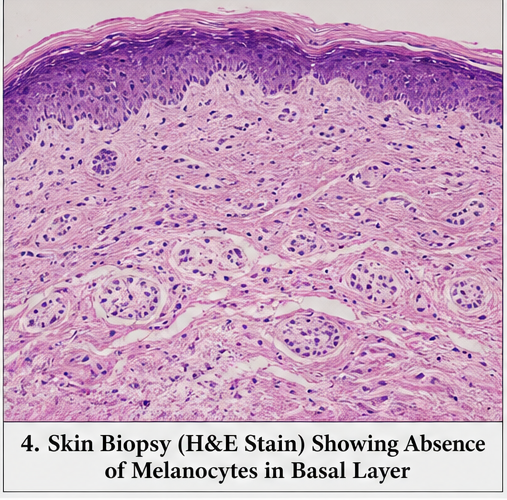
Dermatological Tests
- Skin biopsy (if performed):
- Absence of melanocytes in basal layer
- Mild lymphocytic infiltration
Imaging
- Not required in this case
Diagnosis
A diagnosis of non-segmental vitiligo associated with autoimmune thyroid disease was established based on clinical features, Wood’s lamp findings, and laboratory investigations.
Management and Outcome
Management Strategy
The treatment approach focused on:
- Arresting disease progression
- Inducing repigmentation
- Addressing associated autoimmune conditions
- Improving psychological well-being
Medical Management
- Topical corticosteroids (mid-potency) for localized lesions
- Topical calcineurin inhibitors (tacrolimus) for facial lesions
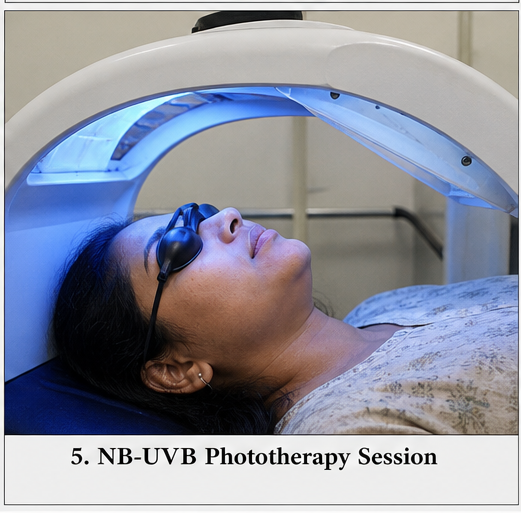
- Narrowband UVB (NB-UVB) phototherapy – 2–3 sessions per week
- Oral antioxidants (vitamins C and E)
Supportive Measures
- Strict photoprotection with broad-spectrum sunscreen
- Counseling regarding chronic nature of disease
- Psychological support for cosmetic concerns
- Monitoring thyroid function and medication adjustment
Clinical Course
During treatment:
- No new lesions developed after 3 months
- Gradual perifollicular repigmentation observed
- Improvement more prominent on facial lesions compared to hands
Follow-Up
At 1 Month
- Stabilization of lesions
- Reduced psychological distress
At 3 Months
- Early repigmentation noted
- No disease progression
At 6 Months
- Approximately 40–50% repigmentation on face
- Minimal response on acral areas
- Good treatment adherence
Discussion
Pathophysiology
Vitiligo is primarily considered an autoimmune disorder characterized by the destruction of melanocytes. Key mechanisms include:
- Autoimmune hypothesis: Cytotoxic T-cell-mediated melanocyte destruction
- Oxidative stress: Accumulation of reactive oxygen species leading to melanocyte damage
- Genetic factors: Association with specific HLA types
- Neural hypothesis: Neurochemical mediators affecting melanocyte survival
These mechanisms act synergistically, leading to progressive depigmentation.
Etiology
Common contributing factors include:
- Autoimmune diseases (e.g., thyroid disorders)
- Genetic predisposition
- Environmental triggers (chemicals, stress)
- Oxidative stress
In this case, autoimmune thyroid disease likely played a significant role.
Epidemiology
- Affects 0.5–2% of the global population
- Equal prevalence in males and females
- Common onset before 30 years of age
- Higher association with autoimmune disorders
Clinical Manifestations
Early Stage
- Small hypopigmented macules
- Often unnoticed
Progressive Stage
- Well-defined depigmented patches
- Symmetrical distribution
- Common sites: face, hands, elbows, knees
Advanced Stage
- Extensive depigmentation
- Leukotrichia
- Mucosal involvement
Diagnostic Considerations
A structured diagnostic approach includes:
- Clinical examination
- Wood’s lamp evaluation
- Laboratory screening for autoimmune disorders
- Skin biopsy (in atypical cases)
Wood’s lamp examination is particularly useful in early or subtle lesions.
Treatment Considerations
Management depends on:
- Extent of disease
- Site of lesions
- Disease activity
- Patient preference
Medical Therapy
- First-line treatment for localized disease
- Includes corticosteroids and calcineurin inhibitors
Phototherapy
- NB-UVB is the gold standard for generalized vitiligo
- Promotes melanocyte proliferation and migration
Surgical Therapy
- Considered in stable vitiligo
- Includes melanocyte transplantation
Emerging Therapies
- Janus kinase (JAK) inhibitors
- Targeted immunomodulators
Complications
Vitiligo is not physically disabling but may lead to:
- Psychological distress
- Social stigma
- Reduced quality of life
- Increased risk of sunburn
Prognosis
The prognosis depends on:
- Disease type (segmental vs non-segmental)
- Duration before treatment initiation
- Site of lesions (face responds better than extremities)
- Patient adherence
Early intervention improves outcomes significantly.
Conclusion
Vitiligo is a chronic dermatological condition with significant psychosocial implications. This case highlights the importance of early recognition and a comprehensive evaluation, particularly for associated autoimmune disorders.
A multimodal treatment approach, including topical therapy and phototherapy, can achieve meaningful repigmentation and disease stabilization. However, treatment responses vary depending on lesion location and disease duration.
Long-term management requires patient education, adherence to therapy, and regular follow-up. Addressing psychological aspects is equally critical in improving overall patient outcomes.
With advancements in targeted therapies, the future of vitiligo management holds promise for more effective and sustained repigmentation strategies.
References
- Taïeb A, Picardo M. Vitiligo. N Engl J Med. https://pubmed.ncbi.nlm.nih.gov/18256395/
- Ezzedine K, Eleftheriadou V, Whitton M, van Geel N. Vitiligo. Lancet. https://pubmed.ncbi.nlm.nih.gov/32171431/
- Bergqvist C, Ezzedine K. Vitiligo: A review. Dermatology. https://pubmed.ncbi.nlm.nih.gov/30235393/
- StatPearls. Vitiligo – Clinical Overview. https://www.ncbi.nlm.nih.gov/books/NBK559149/
- Bolognia JL, Schaffer JV, Cerroni L. Dermatology. https://www.sciencedirect.com/book/9780702062759/dermatology
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge