Typhoid Fever: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Typhoid fever is a systemic infectious disease caused by Salmonella enterica serotype Typhi, characterized by prolonged fever, gastrointestinal symptoms, and potential multisystem complications. It remains a significant public health concern in developing countries due to contaminated food and water. Clinical presentation varies from mild, non-specific symptoms to severe manifestations including intestinal perforation, hemorrhage, and encephalopathy. Diagnosis is primarily clinical, supported by laboratory investigations, blood culture, and serologic testing. Management is focused on prompt antibiotic therapy, supportive care, and prevention of complications. This case report describes a young patient with typhoid fever, highlighting clinical features, diagnostic workup, management, and short-term outcomes. Early diagnosis and timely treatment are crucial to prevent morbidity and mortality.
Introduction
Typhoid fever is an acute systemic infection caused by Salmonella enterica serotype Typhi. It is transmitted through ingestion of contaminated food or water and is endemic in regions with poor sanitation. The global incidence is estimated at 11–21 million cases annually, with approximately 128,000–161,000 deaths.
Clinically, typhoid fever presents with fever, malaise, abdominal discomfort, and gastrointestinal disturbances. Complications such as intestinal perforation, gastrointestinal bleeding, and neuropsychiatric manifestations may occur, particularly in untreated cases. Early recognition and treatment with appropriate antibiotics significantly reduce morbidity and mortality. Despite advances in public health measures, typhoid fever continues to pose diagnostic and therapeutic challenges in endemic areas.
Case Report
Patient History
A 12-year-old male was brought to the pediatric outpatient clinic with a history of persistent high-grade fever for seven days, associated with abdominal pain, malaise, and intermittent headache. The parents reported a recent history of loose stools and mild nausea but no vomiting or jaundice. No history of travel outside the local area was noted.

There was no history of chronic illness, recent antibiotic use, or immunization with typhoid vaccine. Family history was non-contributory. The patient resided in an area with limited access to clean water and had a history of consuming street food occasionally.
Clinical Examination
On physical examination, the patient appeared ill and febrile (temperature 102.8°F). Pulse was 100/min, blood pressure 100/65 mmHg. Abdominal examination revealed mild tenderness in the right lower quadrant without guarding or rebound tenderness. No hepatosplenomegaly was appreciated. The rest of the systemic examination was unremarkable, and neurological status was normal.
Clinical Evaluation
Differential Diagnosis
The differential diagnosis for prolonged fever in a pediatric patient in endemic areas includes:
- Typhoid fever
- Malaria
- Urinary tract infection
- Dengue fever
- Viral hepatitis
Investigations
- Blood tests: CBC revealed mild leukopenia with relative neutropenia and mild anemia. Liver function tests were mildly elevated (AST and ALT).
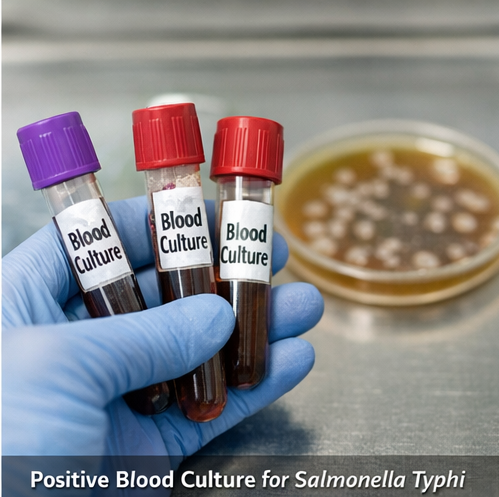
- Blood culture: Positive for Salmonella enterica serotype Typhi, confirming the diagnosis.
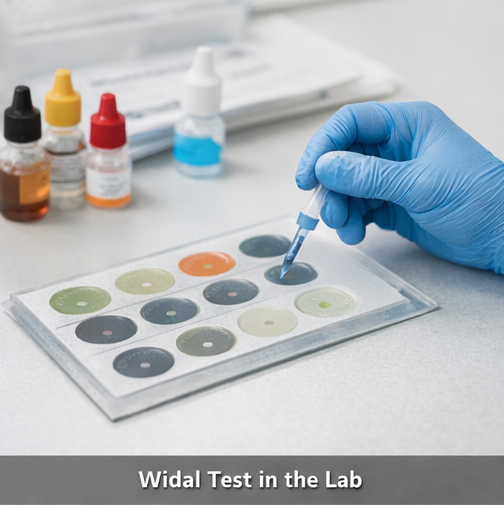
- Widal test: Demonstrated elevated titers of O and H antigens, supportive of the diagnosis in endemic settings.
- Stool and urine cultures: Negative for Salmonella species.
- Imaging: Ultrasound abdomen was normal, with no evidence of bowel perforation or splenomegaly.
Management and Outcome
Management Strategy
The patient was managed with a multidisciplinary approach involving pediatrics and infectious disease specialists. Management included:
- Antibiotic therapy: Oral azithromycin 20 mg/kg once daily for seven days was administered based on local resistance patterns. Intravenous ceftriaxone was considered as an alternative in case of poor oral intake or resistance.

- Supportive care: Adequate hydration, antipyretics for fever, and dietary modifications were implemented.
- Monitoring: Daily vital signs, hydration status, and clinical progress were closely monitored.
- Patient and family education: Counseling was provided on hand hygiene, safe food and water consumption, and recognition of warning signs requiring urgent medical attention.
Follow-Up and Outcome
By the fifth day of antibiotic therapy, the patient became afebrile, appetite improved, and abdominal discomfort resolved. No complications were observed during hospitalization. Blood cultures were negative at follow-up, confirming microbiological clearance. The family was advised regarding preventive measures, including vaccination, clean water access, and hygiene practices. The patient remained well at a two-week outpatient follow-up.
Discussion
Typhoid fever is a preventable and treatable infection, yet it remains a significant health burden in endemic regions. Early diagnosis relies on a high index of suspicion in patients presenting with prolonged fever, gastrointestinal symptoms, and epidemiologic risk factors. Blood culture remains the gold standard for diagnosis, though serologic tests may provide supportive evidence in resource-limited settings.
Prompt initiation of appropriate antibiotics, guided by local resistance patterns, is crucial to prevent complications such as intestinal perforation, hemorrhage, encephalopathy, and relapse. Supportive care, including hydration, nutrition, and antipyretics, complements antimicrobial therapy.
Preventive strategies, including vaccination, improved sanitation, and public health education, are essential to reduce incidence and transmission. Multidisciplinary care involving pediatrics, infectious disease specialists, and public health authorities ensures optimal outcomes. Early treatment, close monitoring, and patient education significantly improve prognosis and reduce morbidity and mortality associated with typhoid fever.
Conclusion
Typhoid fever is a systemic infection caused by Salmonella enterica serotype Typhi, presenting with prolonged fever, abdominal pain, gastrointestinal disturbances, and, in some cases, nonspecific systemic symptoms such as malaise, headache, and anorexia. Early recognition through careful clinical assessment, supported by blood culture, serologic tests, and other laboratory investigations, is essential for differentiating typhoid fever from other causes of prolonged febrile illness in pediatric patients. Prompt initiation of appropriate antibiotic therapy, guided by local resistance patterns, along with supportive care including hydration, nutritional support, and symptom management, significantly reduces the risk of complications such as intestinal perforation, gastrointestinal bleeding, and encephalopathy.
Effective management extends beyond pharmacologic treatment and requires a multidisciplinary approach, involving pediatricians, infectious disease specialists, and public health professionals. Patient and family education on hygiene, safe food and water practices, and recognition of warning signs are critical to prevent recurrence and transmission. Preventive strategies, including vaccination and community-level sanitation improvements, play a key role in reducing disease burden in endemic areas. With timely diagnosis, adherence to therapy, and comprehensive care, pediatric patients can achieve full recovery, avoid severe sequelae, and return to normal growth and development. Long-term follow-up ensures early detection of any relapse or complications and reinforces preventive practices, further improving outcomes and quality of life for affected children.
References
- Parry CM, Hien TT, Dougan G, White NJ, Farrar JJ. Typhoid fever. N Engl J Med. 2002;347:1770–1782.
- Crump JA, Mintz ED. Global trends in typhoid and paratyphoid fever. Clin Infect Dis. 2010;50:241–246.
- Wain J, Hendriksen RS, Mikoleit ML, Keddy KH, Ochiai RL. Typhoid fever. Lancet. 2015;385:1136–1145.
- Ochiai RL, Acosta CJ, Danovaro-Holliday MC, et al. A study of typhoid fever in five Asian countries. Clin Infect Dis. 2008;46(Suppl 1):S1–S17.
- Bhutta ZA. Current concepts in the diagnosis and treatment of typhoid fever. BMJ. 2006;333:78–82.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
PET-CT finds further-reaching metastases in patients with locally advanced breast cancer.
2.
Reasons Behind Refusing Stem Cell Transplantation in Certain Myeloma Patients.
3.
Hospitalization and mortality rates are associated with exposure to the omicron variant of COVID-19 in patients with solid cancer.
4.
AI System Beats Radiologists in Detecting Clinically Significant Prostate Cancer
5.
In heavily pretreated DLBCL, Triplet Scores a Survival Victory.
1.
The Precision Revolution: Bispecific Antibodies and Antibody-Drug Conjugates Reshaping the Oncology Landscape
2.
Is AI The New Radiologist For Breast MRI?
3.
Uncovering New Hope for Follicular Lymphoma Patients
4.
The Silent Signs: Uncovering Stomach Cancer Symptoms Before It's Too Late
5.
Unveiling the Chadwick Sign: A Revolutionary New Tool for Detecting Early Signs of Cancer
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
CDK4/6 Inhibitors Redefining Treatment for HR+/HER2- aBC In Post-Menopausal Women- A Panel Discussion
2.
Efficient Management of First line ALK-rearranged NSCLC - Part V
3.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
4.
Updates on Standard V/S High Risk Myeloma Treatment- The Next Part
5.
Current Cancer Scenario in India- Importance of Genomic Testing & Advancement in Diagnosis and Treatment

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge