Kyrle Disease: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Kyrle disease is a rare acquired perforating dermatosis characterized by transepidermal elimination of abnormal keratin and dermal material. It is most commonly associated with systemic conditions such as chronic kidney disease (CKD) and diabetes mellitus. Clinically, it presents with hyperkeratotic papules and nodules, often accompanied by intense pruritus, predominantly involving the extensor surfaces of the limbs.
We report the case of a 52-year-old male with end-stage renal disease on hemodialysis who presented with multiple pruritic, hyperkeratotic papules over the extremities. Histopathological examination confirmed the diagnosis of Kyrle disease. The patient was managed with a combination of topical keratolytics, systemic retinoids, and optimization of underlying systemic disease, leading to significant symptomatic improvement.
This case underscores the importance of recognizing Kyrle disease as a cutaneous marker of systemic illness and highlights the role of multidisciplinary management in improving patient outcomes.
Introduction
Kyrle disease, first described by Josef Kyrle in 1916, is classified under acquired perforating dermatoses. These conditions are characterized by the elimination of dermal substances through the epidermis, a process termed transepidermal elimination. Kyrle disease is distinct in that it involves keratin debris without significant collagen or elastic fiber extrusion.
The disease is most commonly observed in adults with underlying systemic disorders, particularly chronic renal failure and diabetes mellitus. The exact prevalence is unclear, but it is considered rare and likely underdiagnosed. The pathogenesis is not fully understood, though abnormal keratinization and impaired epidermal turnover are thought to play a central role.
Risk factors for Kyrle disease include:
• Chronic kidney disease, especially patients on dialysis
• Diabetes mellitus
• Liver disease
• Hyperlipidemia
• Genetic predisposition (rare familial cases)
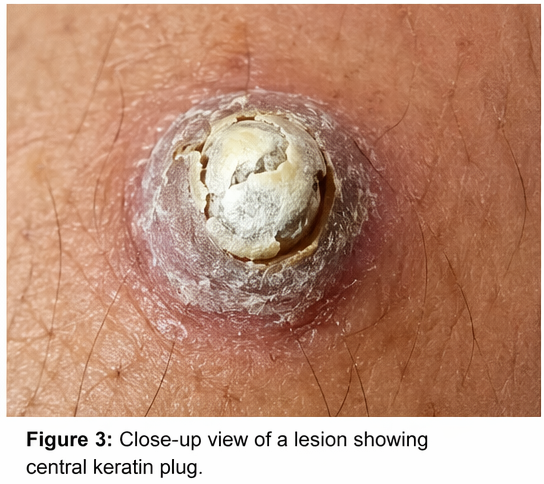
Clinically, Kyrle disease presents as large papules or nodules with central keratin plugs, often associated with severe itching. Lesions commonly occur on the lower extremities but may become generalized. Early diagnosis is essential, as effective management often requires addressing the underlying systemic condition.
Case Report
Patient History
A 52-year-old male presented to the dermatology outpatient department with complaints of:
• Multiple raised skin lesions over the arms and legs for 6 months
• Severe itching, especially at night
• Progressive increase in the number and size of lesions


The patient had a known history of chronic kidney disease and had been on maintenance hemodialysis for the past 3 years. He also had poorly controlled type 2 diabetes mellitus. There was no history of similar skin conditions in the past or in family members.
The pruritus significantly affected his quality of life, leading to sleep disturbance and excoriations.
Clinical Examination
On general examination:
• Patient was afebrile
• Vital signs were stable
• Pallor was present, consistent with chronic disease
Dermatological examination revealed:
• Multiple hyperkeratotic papules and nodules ranging from 3–10 mm
• Lesions with central keratin plugs
• Distribution predominantly over extensor surfaces of forearms and legs
• Evidence of excoriation and post-inflammatory hyperpigmentation
• No mucosal involvement
There were no signs of secondary infection. The rest of the systemic examination was consistent with chronic kidney disease.
Clinical Evaluation
Differential Diagnosis
Based on the clinical presentation, the following conditions were considered:
• Kyrle disease
• Prurigo nodularis
• Lichen planus
• Perforating folliculitis
• Reactive perforating collagenosis
The presence of large keratotic papules with central plugs in a patient with CKD strongly suggested Kyrle disease.
Investigations
Laboratory Findings:
• Hemoglobin: 9.5 g/dL (anemia of chronic disease)
• Serum creatinine: Elevated (consistent with CKD)
• Blood urea nitrogen: Elevated
• HbA1c: 8.9% (poor glycemic control)
• Liver function tests: Within normal limits
Histopathology:
Skin biopsy revealed:
• Hyperkeratosis with parakeratosis
• Epidermal invagination filled with keratin debris
• Transepidermal elimination of keratin material
• Mild inflammatory infiltrate in dermis
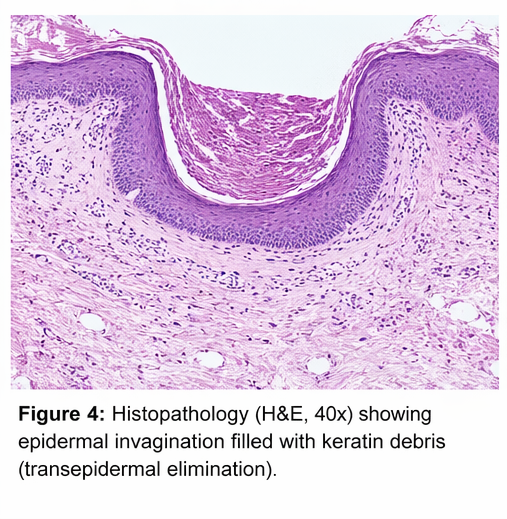
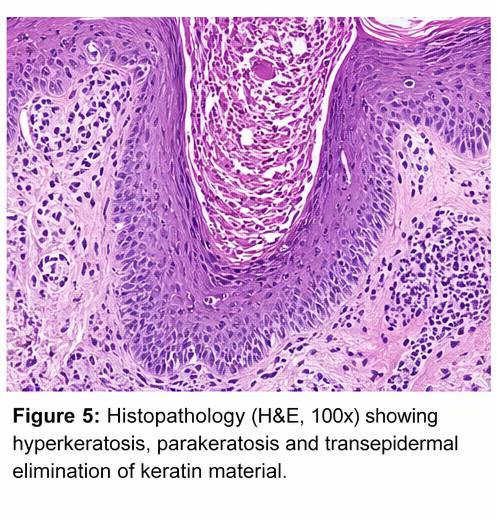
These findings confirmed the diagnosis of Kyrle disease.
Diagnosis
Based on clinical features and histopathological findings, a diagnosis of Kyrle disease was established.
Management and Outcome
Management Strategy
A multidisciplinary approach involving dermatology, nephrology, and endocrinology teams was adopted. The primary goals were:
• Symptom control (pruritus)
• Reduction of skin lesions
• Optimization of underlying systemic disease
Medical Treatment
Topical therapy:
• Keratolytic agents (salicylic acid, urea-based creams)
• Topical retinoids to normalize keratinization
• Emollients to reduce dryness and itching
Systemic therapy:
• Oral retinoids (acitretin) for severe lesions
• Antihistamines for pruritus control
• Optimization of dialysis regimen
• Strict glycemic control
Adjunctive therapy:
• Phototherapy (narrowband UVB) considered in refractory cases
Post-Treatment Course
At 4 weeks:
• Reduction in pruritus intensity
• Flattening of some lesions
At 3 months:
• Significant improvement in skin lesions
• Decrease in new lesion formation
• Improved sleep and quality of life
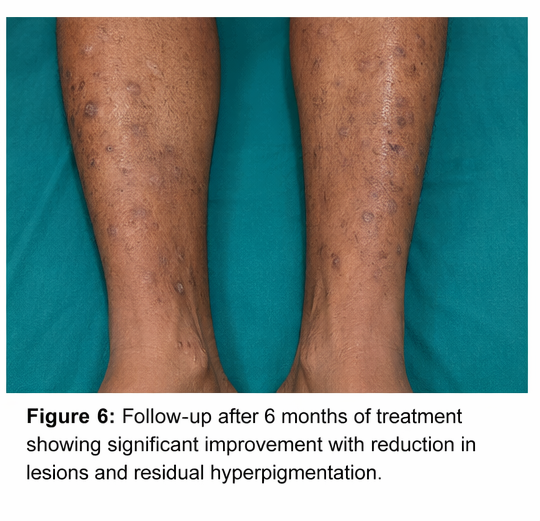
At 6 months:
• Marked reduction in lesion count
• Residual hyperpigmentation present
• No major adverse effects of therapy
The patient demonstrated good compliance and overall favorable response to treatment.
Discussion
Pathophysiology
Kyrle disease is characterized by abnormal keratinization and transepidermal elimination. The process involves:
• Formation of keratin plugs
• Penetration of keratin into the dermis
• Elimination through epidermal invagination
In patients with chronic kidney disease and diabetes, metabolic disturbances may impair epidermal turnover and promote keratin accumulation. Microvascular changes and chronic inflammation may further contribute to disease development.
Diagnostic Challenges
Diagnosis of Kyrle disease can be challenging due to its similarity with other pruritic dermatoses. Key challenges include:
• Overlap with other perforating disorders
• Misdiagnosis as prurigo nodularis
• Lack of awareness due to rarity
Histopathology remains the gold standard for diagnosis.
Treatment Considerations
General principles:
• Treat underlying systemic disease
• Control pruritus
• Reduce keratinization
Therapeutic options:
• Topical keratolytics and retinoids
• Systemic retinoids in severe cases
• Phototherapy
• Dialysis optimization
There is no definitive cure, and management is largely symptomatic and supportive.
Complications
If untreated, Kyrle disease may lead to:
• Severe pruritus and sleep disturbance
• Secondary bacterial infection due to scratching
• Scarring and hyperpigmentation
• Reduced quality of life
Prognosis
The prognosis depends on:
• Control of underlying systemic disease
• Patient compliance with treatment
• Severity of skin involvement
Improvement is often gradual, and recurrence is common if underlying conditions are not well managed.
Conclusion
Kyrle disease is a rare but clinically significant dermatological condition often associated with systemic illnesses such as chronic kidney disease and diabetes mellitus. This case highlights the importance of early recognition, accurate diagnosis through histopathology, and a multidisciplinary approach to management.
Effective treatment requires not only dermatological therapy but also optimization of underlying systemic conditions. With appropriate intervention, patients can achieve significant symptomatic relief and improved quality of life. Increased awareness among clinicians is essential for timely diagnosis and management of this underrecognized condition.
References
- Kyrle, J. (1916). Hyperkeratosis follicularis et parafollicularis in cutem penetrans. Archiv für Dermatologie und Syphilis. https://pubmed.ncbi.nlm.nih.gov/?term=Kyrle+disease+1916
- Rapini, R. P., Herbert, A. A., & Drucker, C. R. (1989). Acquired perforating dermatosis: Evidence for combined transepidermal elimination of both collagen and elastic fibers. Journal of the American Academy of Dermatology. https://pubmed.ncbi.nlm.nih.gov/2645331/
- Saray, Y., & Seçkin, D. (2005). Acquired perforating dermatosis: clinicopathological features in twenty-two cases. Journal of the European Academy of Dermatology and Venereology. https://pubmed.ncbi.nlm.nih.gov/16040378/
- García-Malinis, A. J., et al. (2017). Kyrle disease: a clinical and histopathological study. International Journal of Dermatology. https://pubmed.ncbi.nlm.nih.gov/28294593/
- Morton, C. A., et al. (1996). Acquired perforating dermatosis in patients with renal failure and diabetes mellitus. British Journal of Dermatology. https://pubmed.ncbi.nlm.nih.gov/8864026/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge