Uterine Synechiae (Asherman Syndrome): Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
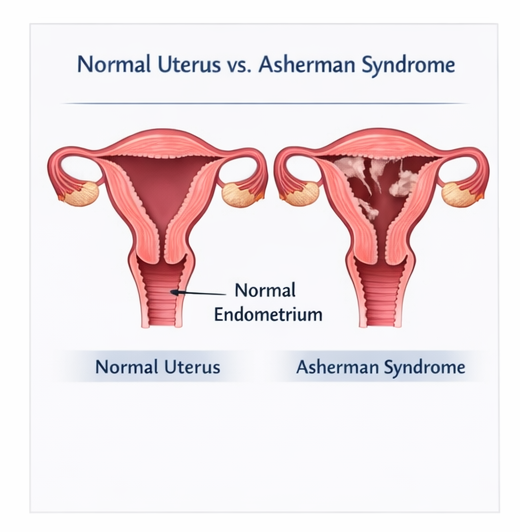
Uterine synechiae, commonly referred to as Asherman syndrome, is a condition characterized by the formation of intrauterine adhesions resulting in partial or complete obliteration of the uterine cavity. It is most frequently associated with trauma to the endometrial lining following uterine instrumentation such as dilation and curettage. Patients typically present with menstrual irregularities, infertility, or recurrent pregnancy loss. Early diagnosis is crucial to restore uterine anatomy and function. Diagnostic modalities include hysteroscopy, hysterosalpingography, and transvaginal ultrasound. Management primarily involves hysteroscopic adhesiolysis followed by hormonal therapy and preventive strategies to reduce recurrence. This case report describes a patient with uterine synechiae presenting with secondary amenorrhea and infertility, outlining the clinical presentation, diagnostic evaluation, and favorable outcome following treatment.
Introduction
Uterine synechiae, or Asherman syndrome, is a significant yet underrecognized cause of secondary amenorrhea and infertility. It is defined by the presence of fibrous adhesions within the uterine cavity resulting from damage to the endometrial basal layer. These adhesions may range from thin filmy bands to dense fibrotic scars leading to complete obliteration of the uterine cavity.
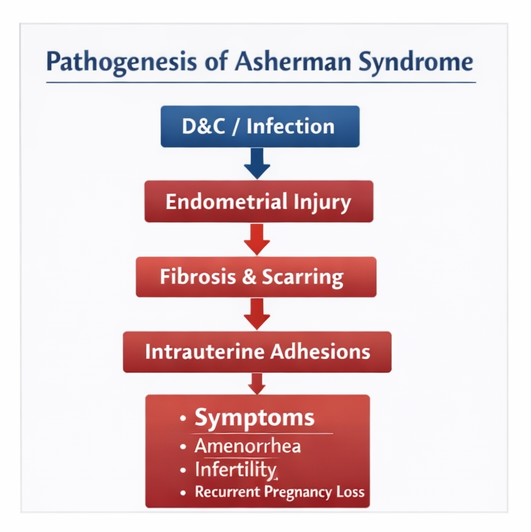
The most common etiology is uterine trauma, particularly following dilation and curettage (D&C) procedures performed after miscarriage, retained products of conception, or postpartum hemorrhage. Other contributing factors include intrauterine infections such as genital tuberculosis, cesarean sections, myomectomy, and radiation exposure.
The pathogenesis involves destruction of the regenerative endometrial layer, leading to fibrosis and adhesion formation between opposing uterine walls. This disrupts normal endometrial regeneration and menstrual function.
Risk factors include:
• Repeated dilation and curettage procedures
• Postpartum uterine instrumentation
• Intrauterine infections (especially tuberculosis in endemic regions)
• Previous uterine surgeries
• Chronic endometrial inflammation
Clinically, patients may present with hypomenorrhea, amenorrhea, infertility, or recurrent pregnancy loss. In severe cases, cyclic pelvic pain may occur due to outflow obstruction.
Early recognition and timely management are essential to restore normal uterine architecture and improve reproductive outcomes.
Case Report
Patient History
A 32-year-old female presented to the gynecology outpatient department with complaints of absence of menstruation for the past six months and inability to conceive for two years.
The patient reported:
• Gradual reduction in menstrual flow over several months progressing to complete amenorrhea
• Mild, intermittent lower abdominal discomfort
• No history of galactorrhea or systemic illness
Her obstetric history revealed a missed abortion at 10 weeks gestation one year prior, for which she underwent dilation and curettage. Following the procedure, she experienced progressively lighter menstrual cycles before eventual cessation.
There was no history suggestive of tuberculosis, pelvic inflammatory disease, or endocrine disorders.
Clinical Examination
On general physical examination, the patient was hemodynamically stable with normal vital parameters.
Pelvic examination findings:
• Normal external genitalia
• Cervix appeared healthy
• Uterus was normal in size, anteverted, and non-tender
• No adnexal masses or cervical motion tenderness
Overall, clinical examination did not reveal any obvious structural abnormalities.
Clinical Evaluation
Differential Diagnosis
Based on the presenting symptoms, the following differential diagnoses were considered:
• Uterine synechiae (Asherman syndrome)
• Hypothalamic-pituitary axis dysfunction
• Premature ovarian insufficiency
• Endometrial atrophy
• Genital tuberculosis
Further investigations were planned to confirm the diagnosis and rule out endocrine causes.
Investigations
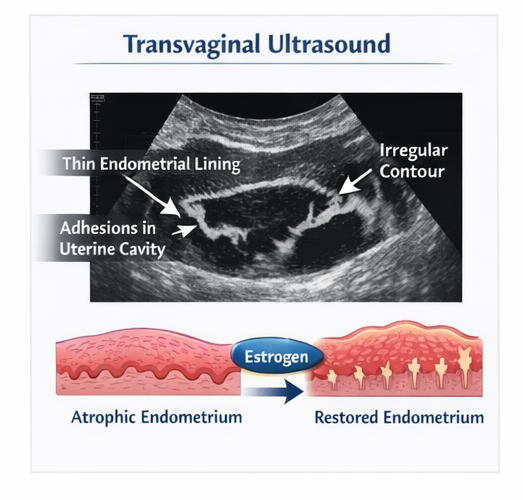
Transvaginal Ultrasound
Ultrasound examination revealed:
• Thin endometrial lining measuring less than expected for phase of cycle
• Irregular endometrial contour
• Suspicion of intrauterine adhesions
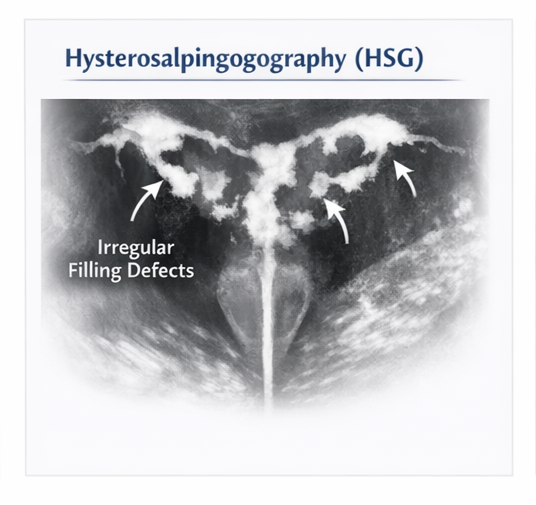
Hysterosalpingography (HSG)
HSG demonstrated:
• Multiple irregular filling defects within the uterine cavity
• Partial obliteration of uterine cavity architecture
• Normal bilateral fallopian tube patency
Diagnostic Hysteroscopy
Hysteroscopy confirmed:
• Presence of dense fibrous adhesions bridging the uterine walls
• Partial obliteration of the uterine cavity
• Poor visualization of the endometrial lining
This established the diagnosis and also allowed assessment of severity.
Laboratory Investigations
• Serum FSH, LH, TSH, and prolactin levels: within normal limits
• Complete blood count: normal
• Tuberculosis screening: negative
Diagnosis
Based on clinical findings and hysteroscopic confirmation, the diagnosis was:
Moderate uterine synechiae (Asherman syndrome)
Management and Outcome
Initial Management
A multidisciplinary plan was formulated involving a gynecologist and fertility specialist.
The treatment strategy included:
• Hysteroscopic adhesiolysis
• Postoperative hormonal therapy
• Measures to prevent adhesion recurrence
Surgical Intervention
The patient underwent hysteroscopic adhesiolysis under direct visualization.
Intraoperative findings:
• Dense fibrous adhesions were identified and carefully dissected
• Restoration of uterine cavity architecture achieved
• Minimal intraoperative bleeding
Postoperative Management
Post-surgical care included:
• High-dose estrogen therapy to promote endometrial regeneration
• Placement of an intrauterine device (temporary) to prevent re-adhesion
• Antibiotic prophylaxis to prevent infection
The patient tolerated the procedure well and was discharged in stable condition.
Follow-Up and Outcome
The patient was followed up over a period of six months.
Outcomes observed:
• Resumption of regular menstrual cycles within two months
• Improved endometrial thickness on follow-up ultrasound
• No recurrence of adhesions on repeat hysteroscopy
At eight months post-treatment, the patient conceived spontaneously and continued antenatal care without complications.
Discussion
Uterine synechiae represents a clinically important cause of secondary amenorrhea and infertility, particularly in women with a history of uterine instrumentation. The condition arises due to damage to the endometrial basal layer, impairing its regenerative capacity and leading to fibrosis.
Dilation and curettage, especially in the setting of pregnancy-related procedures, remains the most common risk factor. In developing regions, genital tuberculosis is also a significant contributor.
The severity of adhesions determines the clinical presentation. Mild cases may present with reduced menstrual flow, whereas severe cases may lead to complete amenorrhea and infertility.
Hysteroscopy is the gold standard for diagnosis, allowing direct visualization and classification of adhesions. It also provides the advantage of simultaneous therapeutic intervention.
Management focuses on:
• Surgical adhesiolysis
• Endometrial regeneration using estrogen therapy
• Prevention of recurrence through mechanical barriers
The prognosis largely depends on the extent of endometrial damage. Mild to moderate cases have good reproductive outcomes, while severe adhesions may result in persistent infertility.
Early detection and intervention significantly improve outcomes, highlighting the importance of clinical suspicion in at-risk patients.
Conclusion
Uterine synechiae is an important and treatable cause of secondary amenorrhea and infertility. A history of uterine instrumentation followed by menstrual abnormalities should prompt evaluation for intrauterine adhesions.
Hysteroscopic adhesiolysis combined with appropriate postoperative management can effectively restore uterine function and improve fertility outcomes.
This case highlights the importance of early diagnosis, multidisciplinary management, and structured follow-up in achieving favorable clinical results.
References
- American College of Obstetricians and Gynecologists (ACOG). Practice guidelines on intrauterine adhesions. https://pmc.ncbi.nlm.nih.gov/articles/PMC5440524/
- March CM. Asherman’s syndrome: current perspectives. Semin Reprod Med. https://pubmed.ncbi.nlm.nih.gov/30936754/
- Schenker JG, Margalioth EJ. Intrauterine adhesions: an updated review. https://pubmed.ncbi.nlm.nih.gov/24373209/
- Yu D, et al. Asherman syndrome—one century later. https://pubmed.ncbi.nlm.nih.gov/24373209/
- Salazar CA, Isaacson KB. Hysteroscopic management of intrauterine adhesions. https://pubmed.ncbi.nlm.nih.gov/28582327/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Does pollution cause cancer?
2.
AI is equally capable of reading breast cancer scans as human radiologists.
3.
EVP Beats Cisplatin for Resectable MIBC
4.
New research points out a promising strategy for treating metastatic medulloblastoma
5.
Academics + Pharma = Big Bucks; New CAR-T Warnings; Patients Seek Cancer Tests.
1.
A Closer Look at Breast Cancer: Examining the Ultrasound Images
2.
Unlocking the Secrets of Oral Cancer Staging: A New Approach to Early Detection
3.
Impact of Hormone Therapy Cessation on Tumor Growth: Case Study of Ki-67 Reduction
4.
Unraveling the Mysteries of Lymphoma: A Journey into the Unknown
5.
Refining AML Survival: Prognostic Factors, Therapies, and Stem Cell Strategies Reviewed
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Navigating the Complexities of Ph Negative ALL - Part III
2.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VIII
3.
Management of 1st line ALK+ mNSCLC (CROWN TRIAL Update)
4.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part III
5.
Virtual Case Study on Pedal Edema and Triple Vessel Disease - An Initiative by Hidoc Dr.

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge