Fibroid Uterus: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Uterine fibroids, also known as leiomyomas, are the most common benign tumors of the female reproductive system, arising from the smooth muscle cells of the myometrium. They are estimated to occur in up to 60–70% of women during the reproductive years, although many remain asymptomatic. Fibroids may vary in size, number, and location within the uterus and can present with symptoms such as abnormal uterine bleeding, pelvic pain, pressure symptoms, infertility, or recurrent pregnancy loss. Diagnosis is primarily based on clinical examination and imaging modalities such as ultrasonography and magnetic resonance imaging (MRI). Management depends on symptom severity, fibroid size and location, and the patient’s reproductive plans. This case report describes a reproductive-age woman presenting with heavy menstrual bleeding and pelvic discomfort, subsequently diagnosed with multiple uterine fibroids through imaging evaluation.
Introduction
Uterine fibroids, medically termed leiomyomas, are benign smooth muscle tumors that originate from the myometrium of the uterus. They represent one of the most common gynecological conditions affecting women of reproductive age. Although the exact etiology remains unclear, fibroid development is influenced by hormonal factors, particularly estrogen and progesterone, as well as genetic and environmental factors.
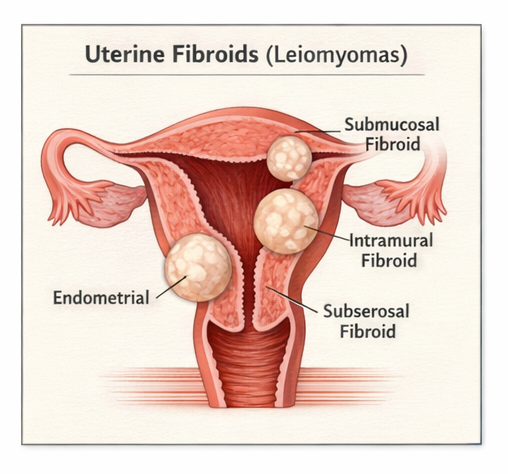
Fibroids are classified according to their location within the uterus: intramural (within the uterine wall), submucosal (protruding into the uterine cavity), and subserosal (extending outward from the uterine surface). The clinical presentation varies depending on the size, number, and location of the fibroids. Many women remain asymptomatic, while others experience significant symptoms such as menorrhagia (heavy menstrual bleeding), pelvic pressure, urinary frequency, infertility, or recurrent miscarriage.
Early recognition is important because untreated symptomatic fibroids can lead to complications such as anemia, infertility, or compression of adjacent pelvic organs. Imaging studies play a critical role in confirming the diagnosis and guiding treatment decisions. This report presents a case of symptomatic uterine fibroids diagnosed through imaging evaluation.
Case Report
Patient History
A 34-year-old female presented to the gynecology outpatient department with complaints of heavy menstrual bleeding for the past six months. The patient reported prolonged menstrual cycles lasting 7–9 days with passage of clots and associated lower abdominal discomfort.
She also complained of pelvic heaviness and occasional urinary frequency. There was no history of intermenstrual bleeding, postcoital bleeding, or significant weight loss. The patient had two previous normal vaginal deliveries and no history of infertility.
Her past medical history was unremarkable, and she was not taking any long-term medications. Family history did not reveal any significant gynecological disorders.
Clinical Examination
The patient appeared mildly pale but otherwise stable.
• Temperature: 36.9°C
• Pulse: 82 beats per minute
• Blood pressure: 116/72 mmHg
• Respiratory rate: 16 breaths per minute
Abdominal examination revealed mild suprapubic fullness without tenderness.
On pelvic examination, the uterus was enlarged to approximately 12-week gestational size with irregular contours. The uterus was firm, mobile, and non-tender. No adnexal masses were palpated.
Clinical Evaluation
Differential Diagnosis
Based on the presenting symptoms and clinical findings, the following differential diagnoses were considered:
• Uterine fibroids (leiomyoma)
• Adenomyosis
• Endometrial hyperplasia
• Ovarian mass
Further diagnostic investigations were performed to establish the cause of symptoms.
Investigations
Laboratory Findings
Routine blood tests revealed mild anemia.
• Hemoglobin: 10.2 g/dL
• Total leukocyte count: 6,500/mm³
• Platelet count: 240,000/mm³
• Thyroid function tests: Normal
• Coagulation profile: Normal
The anemia was attributed to chronic heavy menstrual bleeding.
Imaging
Pelvic Ultrasonography
Transabdominal and transvaginal ultrasound revealed an enlarged uterus with multiple well-defined hypoechoic masses arising from the myometrium. The largest lesion measured approximately 5.2 × 4.8 cm and was located in the anterior uterine wall, consistent with an intramural fibroid.
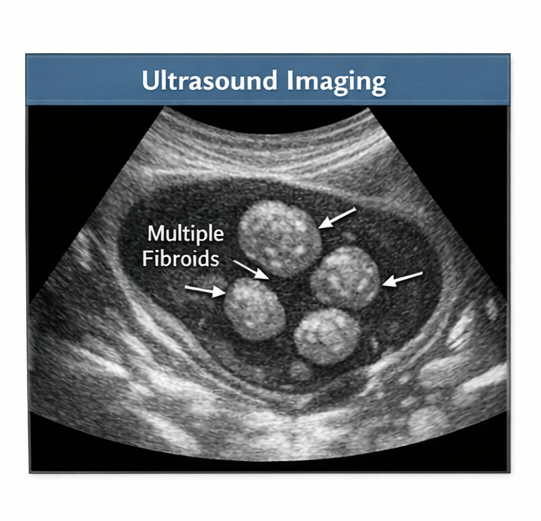
Two smaller fibroids measuring 2–3 cm were noted in the posterior wall and fundal region. The endometrial cavity was mildly distorted but not significantly compressed. Both ovaries appeared normal.
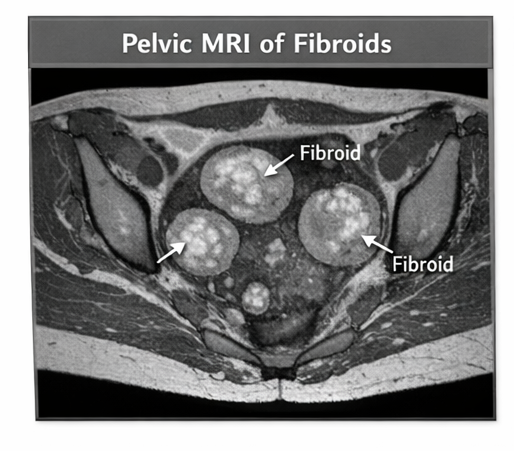
Magnetic Resonance Imaging (MRI)
Pelvic MRI was performed to further characterize the fibroids. MRI confirmed multiple intramural fibroids with well-circumscribed margins and typical low signal intensity on T2-weighted images. No evidence of degeneration or malignancy was identified.
Diagnosis
Based on clinical examination and imaging findings, a diagnosis of symptomatic uterine fibroids (multiple intramural leiomyomas) was established.
Management and Outcome
Clinical Management
The treatment plan was individualized based on the patient’s symptoms and desire for future fertility.
Initial management included:
• Iron supplementation for anemia
• Nonsteroidal anti-inflammatory drugs (NSAIDs) for pain relief
• Hormonal therapy using a combined oral contraceptive to reduce menstrual bleeding
Because the patient desired future fertility, conservative management was initially preferred.
After counseling regarding available treatment options, including myomectomy and uterine artery embolization, the patient elected to undergo laparoscopic myomectomy due to persistent symptoms.
Surgical Findings
During laparoscopic surgery, multiple intramural fibroids were identified within the anterior and posterior uterine walls. The largest fibroid measuring approximately 5 cm was successfully removed along with two smaller fibroids.
The uterine wall was repaired in layers to preserve uterine integrity.
Follow-Up and Outcome
The postoperative period was uneventful. The patient was discharged on the third postoperative day.
At follow-up after three months, the patient reported significant improvement in menstrual bleeding and pelvic discomfort. Hemoglobin levels improved to 12.1 g/dL.
Ultrasound performed during follow-up demonstrated a normal postoperative uterine contour with no residual fibroids.
Discussion
Uterine fibroids are the most common benign tumors of the female reproductive tract. Their prevalence increases with age during reproductive years and decreases after menopause due to declining hormone levels.
Several factors influence fibroid development, including genetic predisposition, hormonal stimulation, and growth factors. Estrogen and progesterone play a significant role in fibroid growth, which explains why fibroids tend to enlarge during pregnancy and regress after menopause.
Clinical manifestations depend on fibroid size, number, and location. The most common symptoms include heavy menstrual bleeding, pelvic pain, pelvic pressure, infertility, and urinary symptoms due to compression of adjacent organs.
Ultrasonography is considered the first-line imaging modality for diagnosing fibroids due to its accessibility and cost-effectiveness. MRI provides more detailed information regarding fibroid size, location, and degeneration, especially when surgical intervention is being considered.
Treatment options vary from conservative medical management to surgical procedures. Medical therapies include hormonal contraceptives, gonadotropin-releasing hormone (GnRH) agonists, and antifibrinolytic agents. Surgical options include myomectomy, hysterectomy, and minimally invasive procedures such as uterine artery embolization.
For women desiring future fertility, myomectomy remains the preferred surgical treatment.
Conclusion
Fibroid uterus is a common gynecological condition that can significantly affect a woman’s quality of life due to symptoms such as heavy menstrual bleeding and pelvic discomfort. Early recognition through clinical examination and imaging studies is important for appropriate management. Treatment should be individualized based on symptom severity, fibroid characteristics, and reproductive goals. With timely diagnosis and appropriate intervention, most patients experience significant symptom relief and favorable outcomes.
References
- Stewart EA. Uterine fibroids. Lancet. 2015.\ https://pubmed.ncbi.nlm.nih.gov/25456052/
- Bulun SE. Uterine fibroids. N Engl J Med. 2013. https://pubmed.ncbi.nlm.nih.gov/23984720/
- Laughlin-Tommaso SK, Stewart EA. Moving toward individualized medicine for uterine fibroids. Obstet Gynecol Clin North Am. 2016. https://pubmed.ncbi.nlm.nih.gov/27261815/
- Parker WH. Etiology, symptomatology, and diagnosis of uterine myomas. Fertil Steril. 2007. https://pubmed.ncbi.nlm.nih.gov/17583712/
- Dueholm M. Uterine fibroid embolization and other minimally invasive treatments. Best Pract Res Clin Obstet Gynaecol. 2018. https://pubmed.ncbi.nlm.nih.gov/29395112/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Year in Review: Chronic Lymphocytic Leukemia
2.
According to a study, white Americans are overdiagnosing melanoma at an alarming rate.
3.
Approval in Endometrial Cancer Expanded; Masks at Cancer Centers; NPR Reporter Dies
4.
The First Gene Therapy Provides a Durable Response for Non-Muscle-Invasive Bladder Cancer.
5.
Canine Cancer Vaccine: A Potential Resurrection? U.S. KK. Snubs Enertu.
1.
What Is Carboxyhemoglobin And How Can It Affect Your Health?
2.
Lu-177 Vipivotide in Prostate Cancer: A Breakthrough in Radioligand Therapy
3.
Unraveling the Mysteries of Coagulopathy: A Comprehensive Definition
4.
Machine Learning in Genomic Analysis for Early Lung Cancer Detection: Key Advances and Insights
5.
A New Perspective on Spherocytosis: Uncovering Innovative Treatments
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Revolutionizing Treatment of ALK Rearranged NSCLC with Lorlatinib - Part II
2.
Navigating the Complexities of Ph Negative ALL - Part XIII
3.
Updates on the First Line Management of ALK+ NSCLC
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
Breaking Ground: ALK-Positive Lung Cancer Front-Line Management - Part II

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge