Maculopathy: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Maculopathy refers to a spectrum of disorders affecting the macula, the central portion of the retina responsible for high-resolution vision. It is a major cause of visual impairment worldwide, particularly in individuals with systemic risk factors such as diabetes mellitus. Patients commonly present with blurred central vision, metamorphopsia, and difficulty performing tasks requiring fine visual acuity. Diagnosis is based on clinical examination and imaging modalities including optical coherence tomography (OCT) and fundus photography. Early detection and appropriate management are essential to prevent irreversible visual loss. This report describes a case of diabetic maculopathy in a middle-aged patient that was successfully diagnosed and managed with intravitreal therapy and systemic control.
Introduction
Maculopathy encompasses a range of pathological conditions involving the macula, leading to impairment of central vision. Among these, diabetic maculopathy is one of the most common causes, particularly in patients with long-standing or poorly controlled diabetes mellitus.
The underlying pathophysiology involves microvascular damage, breakdown of the blood-retinal barrier, and increased vascular permeability, resulting in accumulation of fluid and lipids in the macular region. This leads to retinal thickening and disruption of photoreceptor function, ultimately affecting visual acuity.
Other causes of maculopathy include age-related macular degeneration (AMD), central serous chorioretinopathy, and drug-induced retinal toxicity. Risk factors include chronic hyperglycemia, hypertension, dyslipidemia, smoking, and increasing age.
Clinical presentation typically includes gradual blurring of vision, distortion of images (metamorphopsia), and difficulty in reading or recognizing faces. Early identification using advanced imaging techniques such as OCT is crucial for diagnosis and monitoring response to therapy.
This report presents a case of diabetic maculopathy diagnosed in a patient with visual complaints and highlights the importance of early intervention and multidisciplinary management.
Case Report
Patient History
A 52-year-old female presented to the ophthalmology outpatient department with complaints of gradual, painless diminution of vision in the right eye over a period of two months.
The patient reported difficulty in reading fine print and noticed distortion of straight lines, particularly while reading text. There was no history of redness, photophobia, floaters, or ocular trauma.
She had a known history of type 2 diabetes mellitus for the past 8 years, with irregular medication adherence and poor glycemic control. There was no history of hypertension, renal disease, or previous ocular interventions.
Clinical Examination
On general examination, the patient was stable and afebrile.
Ocular examination findings were as follows:
• Best corrected visual acuity: 6/18 in the right eye and 6/9 in the left eye
• Intraocular pressure: within normal limits in both eyes
• Anterior segment examination: normal
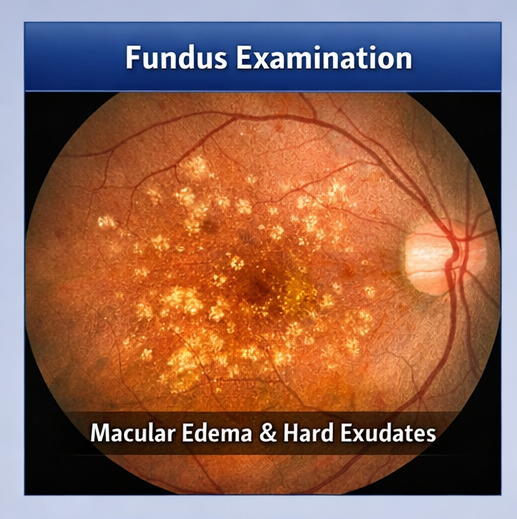
Fundus examination of the right eye revealed macular thickening with the presence of hard exudates and microaneurysms in the central retina. The left eye fundus appeared normal.
Clinical Evaluation
Differential Diagnosis
Based on the clinical findings, the following differential diagnoses were considered:
• Diabetic maculopathy
• Age-related macular degeneration
• Central serous chorioretinopathy
• Drug-induced maculopathy
Further diagnostic investigations were carried out to confirm the diagnosis.
Investigations
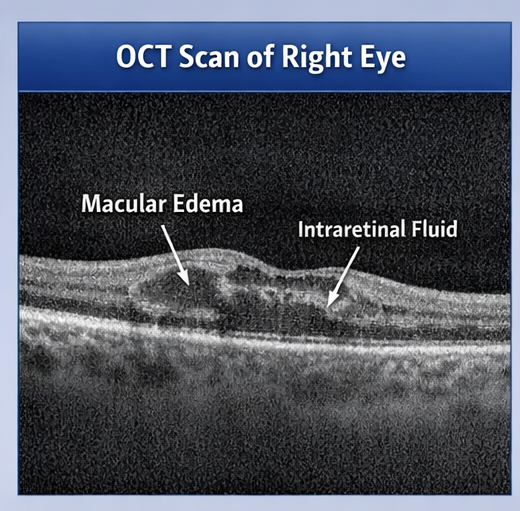
Optical Coherence Tomography (OCT)
OCT of the right eye demonstrated increased central macular thickness with intraretinal cystic spaces, indicating macular edema.
Fundus Photography
Fundus imaging showed the presence of hard exudates and microaneurysms in the macular region.
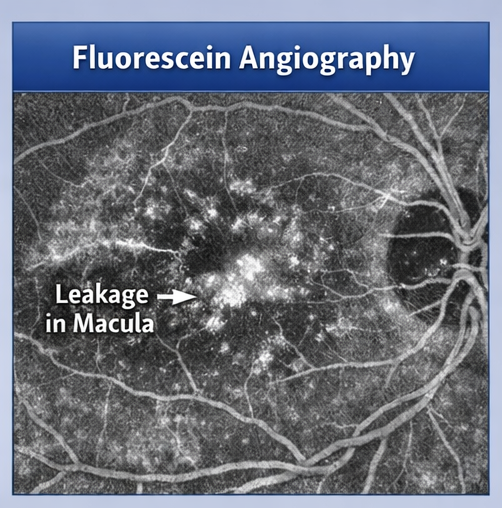
Fluorescein Angiography
Fluorescein angiography revealed focal areas of leakage in the macula, consistent with diabetic macular edema.
Laboratory Investigations
• Glycated hemoglobin (HbA1c): 8.5% (elevated)
• Serum creatinine: within normal limits
• Lipid profile: mildly elevated
Diagnosis
Based on clinical findings and imaging studies, along with a history of poorly controlled diabetes, a diagnosis of diabetic maculopathy with macular edema was established.
Management and Outcome
Initial Management
The patient was initiated on the following management plan:
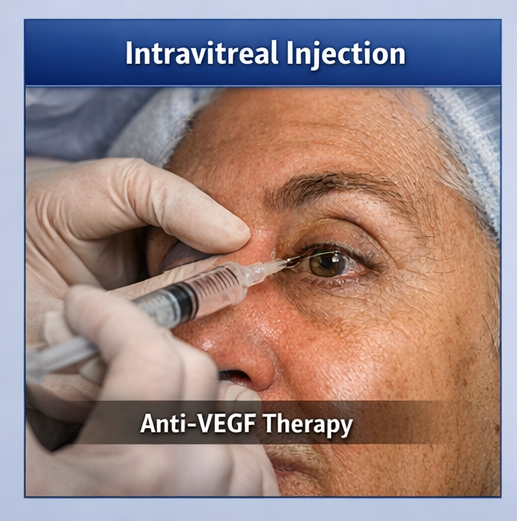
• Intravitreal anti-vascular endothelial growth factor (anti-VEGF) injections
• Optimization of glycemic control in consultation with a physician
• Dietary modification and lifestyle counseling
• Regular follow-up with OCT monitoring
Follow-Up and Outcome
The patient was followed up at regular intervals over a period of three months.
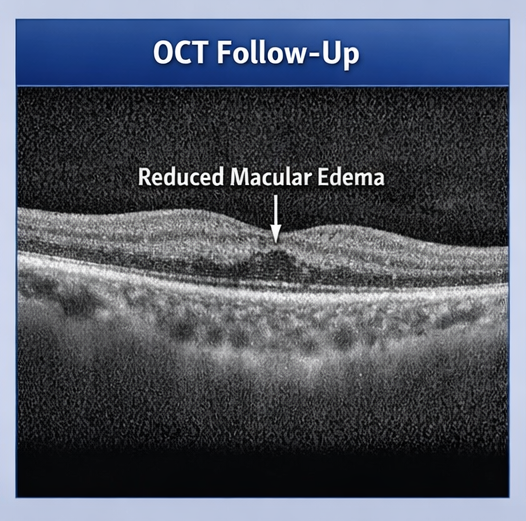
After initiation of intravitreal anti-VEGF therapy, there was a gradual improvement in visual symptoms. The patient reported reduction in visual distortion and improved ability to read.
Repeat OCT imaging demonstrated a significant reduction in macular edema, with decreased retinal thickness and resolution of intraretinal fluid.
Visual acuity improved from 6/18 to 6/9 in the affected eye.
Glycemic control was also improved with better adherence to antidiabetic therapy, reflected by a reduction in HbA1c levels on subsequent evaluation.
At the end of three months, the patient remained clinically stable with no progression of disease. Continued follow-up and maintenance therapy were advised.
Discussion
Maculopathy, particularly diabetic maculopathy, is a leading cause of visual impairment in the working-age population. It represents a microvascular complication of diabetes characterized by increased vascular permeability, capillary leakage, and retinal edema.
The development of diabetic macular edema is closely linked to chronic hyperglycemia, which leads to endothelial dysfunction and disruption of the blood-retinal barrier. Accumulation of fluid and lipid exudates in the macula results in retinal thickening and impaired visual function.
Clinically, patients present with gradual, painless loss of central vision and metamorphopsia. Early stages may be asymptomatic, highlighting the importance of routine screening in diabetic patients.
Optical coherence tomography has become the gold standard for diagnosis and monitoring, as it provides high-resolution cross-sectional imaging of the retina. Fluorescein angiography is useful in identifying areas of leakage and guiding treatment.
Management strategies focus on reducing macular edema and preventing progression. Intravitreal anti-VEGF agents are the mainstay of treatment and have been shown to significantly improve visual outcomes. Laser photocoagulation may be considered in selected cases.
Systemic control of diabetes, hypertension, and dyslipidemia is equally important in preventing progression and recurrence. Multidisciplinary care involving ophthalmologists and physicians plays a key role in optimal patient outcomes.
Early detection and timely intervention are critical in preserving vision and improving quality of life.
Conclusion
Maculopathy is a significant cause of central vision loss, particularly in patients with diabetes mellitus.
Early diagnosis through clinical examination and imaging modalities such as OCT is essential for effective management.
Intravitreal anti-VEGF therapy, combined with optimal systemic control, remains the cornerstone of treatment.
With timely intervention and regular follow-up, favorable visual outcomes can be achieved, as demonstrated in this case.
References
- American Academy of Ophthalmology. Diabetic Retinopathy Preferred Practice Pattern. https://pubmed.ncbi.nlm.nih.gov/33220753/
- Browning DJ, et al. Diabetic macular edema: pathophysiology and management. https://pubmed.ncbi.nlm.nih.gov/28494911/
- Ferris FL, et al. Clinical classification of diabetic retinopathy. https://pubmed.ncbi.nlm.nih.gov/14972475/
- Wong TY, et al. Diabetic retinopathy. Nature Reviews Disease Primers. https://pubmed.ncbi.nlm.nih.gov/28758912/
- Schmidt-Erfurth U, et al. Guidelines for the management of diabetic macular edema. https://pubmed.ncbi.nlm.nih.gov/27001244/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Researchers find distinct cell receptors with the potential for new treatments.
2.
Breast cancer patients' arms swell less after an effective lymph node transfer.
3.
Telehealth in the pandemic era resulted in fewer therapy interruptions.
4.
Too Many Chest CTs for Incidental Lung Nodules?
5.
Global warming could be driving up women's cancer risk, find researchers
1.
The New Frontier of Cancer Survivorship: Navigating the Long-Term Effects of Immunotherapy and Targeted Therapies
2.
Deterministic Reprogramming of Neutrophils within Tumors: A New Frontier in Cancer Research
3.
Neuroendocrine Tumors: Case Study on Diagnosis, Treatment Strategies & Patient Management
4.
Ticagrelor Monotherapy vs. Ticagrelor + Aspirin in ACS Post-PCI: ULTIMATE-DAPT Trial
5.
Transfusing the Future: Exploring the Possibilities of Blood Transfusions
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Current Scenario of Blood Cancer- A Conclusion on Genomic Testing & Advancement in Diagnosis and Treatment
2.
Navigating the Brain Barrier: The CNS Challenge in ALK+ NSCLC
3.
Thromboprophylaxis In Medical Settings
4.
Treatment Paradigm for Patients with R/R Adult B-cell ALL- Expert Discussions
5.
Current Scenario of Blood Cancer- Genomic Testing & Advancement in Diagnosis and Treatment

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge