Aphhthous Ulcer Stomatitis: Clinical Presentation, Diagnostic Evaluation, Management, And Outcomes – A Case Report
OthersPage Navigation
Abstract
Recurrent aphthous stomatitis (RAS), commonly referred to as aphthous ulcer stomatitis, is a prevalent chronic inflammatory condition of the oral mucosa characterized by recurrent, painful ulcerations. Although benign and self-limiting, the condition significantly affects oral intake, speech, and quality of life. The etiology is multifactorial, involving immune dysregulation, nutritional deficiencies, genetic predisposition, and local triggers.
We report the case of a 32-year-old female presenting with recurrent painful oral ulcers for 6 months, affecting eating and daily activities. Clinical examination revealed multiple shallow ulcers with erythematous halos on the buccal mucosa and tongue. Laboratory investigations indicated iron deficiency and low vitamin B12 levels. The patient was managed with topical corticosteroids, oral supplements, and supportive care, resulting in symptomatic relief and reduced recurrence frequency.
This case emphasizes the importance of identifying underlying systemic factors, implementing targeted therapy, and adopting a holistic management approach in recurrent aphthous stomatitis.
Introduction
Recurrent aphthous stomatitis (RAS) is one of the most common disorders affecting the oral mucosa, with a prevalence ranging from 5% to 25% in the general population. It is characterized by recurrent episodes of painful, round or oval ulcers with a yellowish base and erythematous margins, typically affecting non-keratinized mucosal surfaces such as the buccal mucosa, labial mucosa, and tongue.
RAS is broadly classified into three types: minor, major, and herpetiform ulcers. Minor aphthae are the most common, accounting for approximately 80–85% of cases. The condition usually begins in childhood or adolescence and tends to decrease in frequency with age.
The exact pathogenesis remains unclear but is believed to involve a T-cell-mediated immune response leading to mucosal destruction. Contributing factors include nutritional deficiencies (iron, vitamin B12, folate), stress, hormonal changes, food sensitivities, and systemic conditions such as celiac disease and inflammatory bowel disease.
Despite its benign nature, RAS can significantly impair quality of life due to pain and recurrent episodes. Early recognition and identification of underlying causes are essential for effective management and prevention of recurrence.
Case Report
Patient History
A 32-year-old female presented to the outpatient department with:
- Recurrent painful oral ulcers for 6 months
- Difficulty in eating and speaking during episodes
- Burning sensation in the oral cavity
- Ulcers recurring every 3–4 weeks
There was no history of fever, weight loss, or systemic illness. The patient reported increased stress levels due to occupational factors.
Medical history revealed no chronic diseases. There was no history of similar lesions in childhood.
Dietary history suggested inadequate intake of green leafy vegetables and animal protein. There was no history of tobacco or alcohol use.
Family history was non-contributory.
Clinical Examination
General Examination
- Patient conscious and oriented
- Vitals stable
- Mild pallor noted
Oral Examination
- Multiple round to oval ulcers measuring 3–5 mm
- Location: buccal mucosa, lateral border of tongue, and inner lip
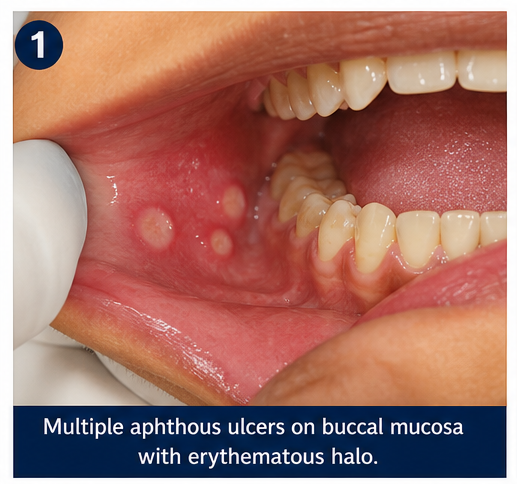
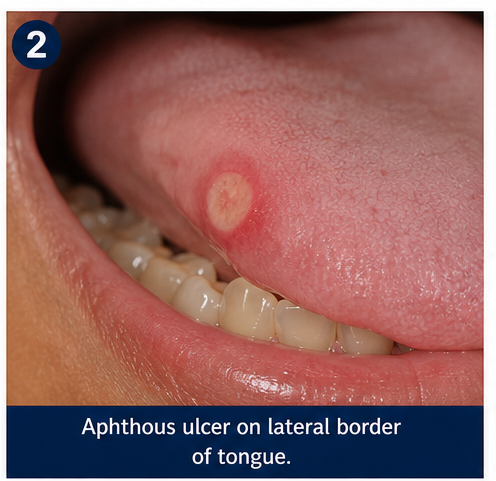
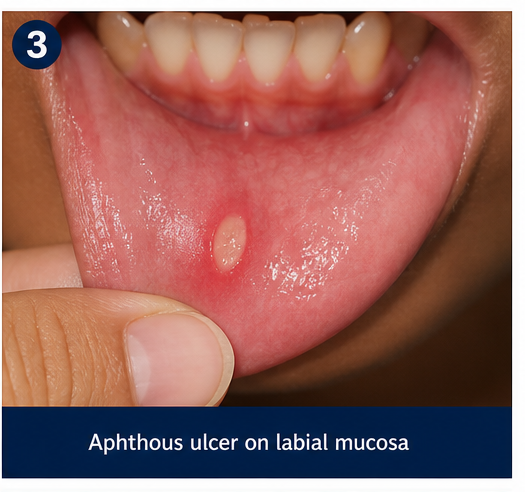
- Ulcers with yellowish base and erythematous halo
- Tender on palpation
- No induration or bleeding
- No vesicles or crusting
Systemic Examination
- No significant abnormalities detected
Clinical Evaluation
Differential Diagnosis
Based on clinical presentation, the following were considered:
- Recurrent aphthous stomatitis (most likely)
- Herpetic stomatitis
- Oral candidiasis
- Lichen planus
- Traumatic ulcers
The absence of vesicles, fungal plaques, and systemic symptoms favored a diagnosis of aphthous ulcers.
Investigations
Laboratory Tests
- Complete blood count: Mild anemia
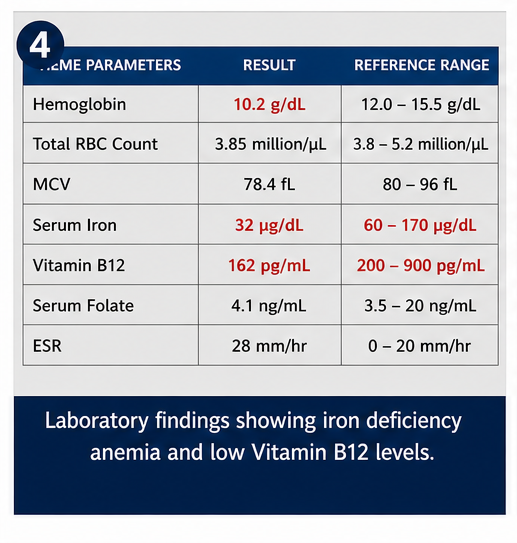
- Serum iron: Reduced
- Vitamin B12: Low
- Serum folate: Borderline low
- Blood glucose: Normal
- ESR: Mildly elevated
Other Tests
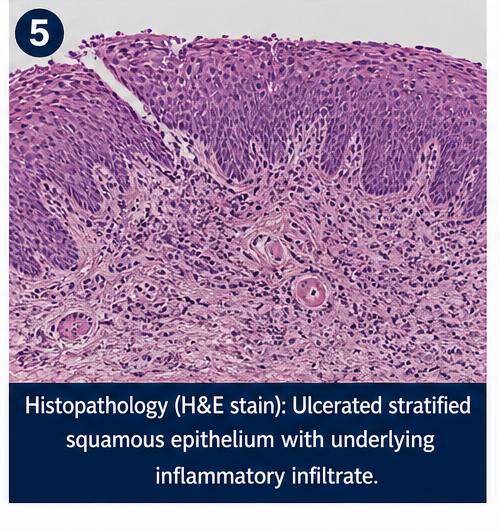
- No biopsy required (typical presentation)
Diagnosis
A diagnosis of recurrent aphthous stomatitis (minor type) associated with nutritional deficiency was established based on clinical features and laboratory findings.
Management and Outcome
Management Strategy
The treatment plan focused on:
- Pain relief
- Reduction of ulcer duration
- Prevention of recurrence
- Correction of nutritional deficiencies
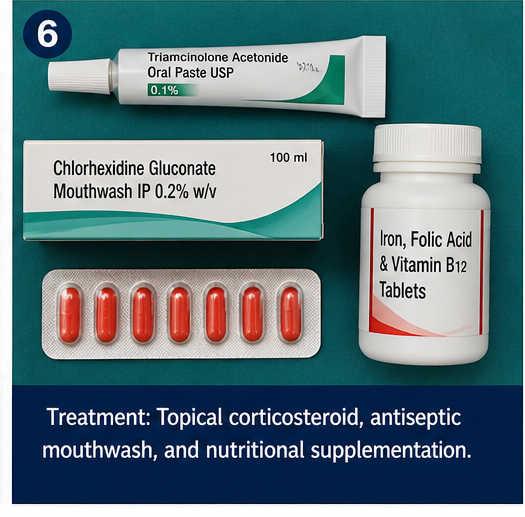
Medical Management
- Topical corticosteroids (triamcinolone acetonide oral paste)
- Topical anesthetic gel (lidocaine) for pain relief
- Antiseptic mouthwash (chlorhexidine)
- Oral iron supplementation
- Vitamin B12 and folic acid supplements
Supportive Measures
- Avoidance of spicy and acidic foods
- Maintenance of oral hygiene
- Stress management techniques
- Adequate hydration
- Dietary counseling
Clinical Course
During treatment:
- Pain reduced within 3–5 days
- Ulcers healed within 10–14 days
- Frequency of recurrence decreased over time
Follow-Up
At 1 Month
- Reduced severity of ulcers
- Improved oral intake
At 3 Months
- Fewer episodes reported
- Nutritional parameters improving
At 6 Months
- Significant reduction in recurrence frequency
- Occasional mild ulcers only
Discussion
Pathophysiology
RAS is considered an immune-mediated condition involving T-cell activation and cytokine release, leading to epithelial damage.
Key mechanisms include:
- Immune dysregulation
- Increased TNF-alpha levels
- Mucosal barrier breakdown
- Nutritional deficiencies affecting epithelial integrity
Etiology
Contributing factors include:
- Nutritional deficiencies (iron, vitamin B12, folate)
- Stress and psychological factors
- Hormonal changes
- Food hypersensitivity
- Genetic predisposition
In this case, nutritional deficiency and stress were significant contributors.
Epidemiology
- Prevalence: 5–25% globally
- More common in females
- Peak incidence in young adults
- Decreases with age
Clinical Manifestations
Minor Aphthae
- Small ulcers (<1 cm)
- Heal without scarring
Major Aphthae
- Larger, deeper ulcers
- May scar
Herpetiform Ulcers
- Multiple small ulcers
- May coalesce
Diagnostic Considerations
Diagnosis is primarily clinical and includes:
- Detailed history
- Oral examination
- Nutritional assessment
- Laboratory tests (if recurrent or severe)
Biopsy is reserved for atypical or non-healing ulcers.
Treatment Considerations
Topical Therapy
- First-line treatment
- Includes corticosteroids and anesthetics
Systemic Therapy
- For severe or refractory cases
- Includes corticosteroids, colchicine, or immunomodulators
Nutritional Therapy
- Essential in deficiency states
- Improves outcomes
Emerging Therapies
- Biologic agents targeting TNF-alpha
- Laser therapy
- Probiotics
Complications
Although benign, RAS can lead to:
- Nutritional compromise due to pain
- Psychological distress
- Reduced quality of life
Prognosis
The prognosis is generally good, with most cases resolving spontaneously. However, recurrence is common.
Factors influencing prognosis:
- Frequency of episodes
- Underlying deficiencies
- Patient compliance
- Stress levels
Conclusion
Recurrent aphthous stomatitis is a common yet often distressing oral condition with multifactorial etiology. This case highlights the importance of a comprehensive approach, including identification of underlying nutritional deficiencies and appropriate therapeutic intervention.
Topical therapy combined with nutritional supplementation and lifestyle modification can significantly reduce symptom severity and recurrence. Patient education and regular follow-up are crucial for long-term management.
With ongoing research into immunological pathways and targeted therapies, future treatment strategies may offer more definitive control of this recurrent condition.
References
- Taïeb A, Picardo M. Vitiligo. N Engl J Med. https://pubmed.ncbi.nlm.nih.gov/18256395/
- Ezzedine K, Eleftheriadou V, Whitton M, van Geel N. Vitiligo. Lancet. https://pubmed.ncbi.nlm.nih.gov/32171431/
- Bergqvist C, Ezzedine K. Vitiligo: A review. Dermatology. https://pubmed.ncbi.nlm.nih.gov/30235393/
- StatPearls. Aphthous Ulcers – Clinical Overview. https://www.ncbi.nlm.nih.gov/books/NBK559149/
- Preeti L, Magesh KT, Rajkumar K, Karthik R. Recurrent aphthous stomatitis. https://pubmed.ncbi.nlm.nih.gov/20379402/
- Scully C, Porter S. Oral mucosal disease: Recurrent aphthous stomatitis. https://pubmed.ncbi.nlm.nih.gov/12849283/
- Ship JA. Recurrent aphthous stomatitis: An update. https://pubmed.ncbi.nlm.nih.gov/12436867/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge