Acute Infective Endocarditis in an Intravenous Drug User: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Acute infective endocarditis (IE) is a life-threatening infection of the endocardial surface of the heart, most commonly involving the cardiac valves. Intravenous drug use (IVDU) is a well-recognized risk factor for IE due to repeated bacteremia from non-sterile injection practices. Acute IE in this population is frequently caused by Staphylococcus aureus and commonly affects the right-sided heart valves, particularly the tricuspid valve. Clinical presentation may be nonspecific, with fever being the most common symptom, often leading to delayed diagnosis. Prompt recognition, accurate diagnosis using microbiological and echocardiographic evaluation, and timely initiation of targeted antimicrobial therapy are critical to reduce morbidity and mortality. This case report describes an adult intravenous drug user presenting with acute infective endocarditis, highlighting clinical features, diagnostic approach, management strategies, and short-term outcomes, while emphasizing the importance of early diagnosis and multidisciplinary care.
Introduction
Infective endocarditis is a severe infectious condition characterized by microbial infection of the heart valves or endocardial surface. Despite advances in diagnostic imaging and antimicrobial therapy, IE remains associated with high morbidity and mortality. The epidemiology of IE has evolved over recent decades, with intravenous drug use emerging as a significant predisposing factor, particularly among younger adults.
IV drug users are at increased risk due to repeated venous access, use of contaminated needles, injection of particulate matter, and poor hygienic practices, leading to transient or sustained bacteremia. Right-sided endocarditis, especially involving the tricuspid valve, is more common in this population, although left-sided involvement may also occur.
Acute IE typically presents with systemic symptoms such as fever, chills, and malaise, along with cardiac and extracardiac manifestations. Delayed diagnosis can result in severe complications, including septic emboli, heart failure, and systemic infection. This case report illustrates the clinical course of acute infective endocarditis in an IV drug user, focusing on diagnostic challenges, treatment, and outcomes.
Case Report
Patient History
A 32-year-old male presented to the emergency department with complaints of high-grade fever, chills, and generalized weakness for five days. He also reported pleuritic chest pain and shortness of breath for two days. There was no history of cough, hemoptysis, or prior cardiac disease.
The patient admitted to active intravenous heroin use for the past six years, with frequent needle sharing. He had no known history of valvular heart disease, diabetes mellitus, or immunosuppressive conditions. There was no prior history of infective endocarditis. The patient was not on any regular medications.
Clinical Examination
On examination, the patient appeared acutely ill and febrile. Vital signs revealed a temperature of 39.2°C, heart rate of 118 beats per minute, blood pressure of 104/62 mmHg, respiratory rate of 24 breaths per minute, and oxygen saturation of 95% on room air.
Cardiovascular examination revealed a new systolic murmur best heard at the lower left sternal border, which increased with inspiration. There were no signs of heart failure. Respiratory examination revealed scattered crackles at both lung bases. Examination of the extremities showed multiple healed and fresh injection marks over the forearms.

No peripheral stigmata of endocarditis, such as Janeway lesions or Osler nodes, were noted. Abdominal and neurological examinations were unremarkable.
Clinical Evaluation
Differential Diagnosis
Based on the clinical presentation, the following differential diagnoses were considered:
• Acute infective endocarditis
• Community-acquired pneumonia with sepsis
• Septic pulmonary embolism
• Acute viral febrile illness
• Pulmonary embolism
The combination of persistent fever, IV drug use, new cardiac murmur, and respiratory symptoms raised strong suspicion for acute infective endocarditis.
Investigations
Laboratory Tests:
• Complete blood count: Leukocytosis with neutrophilia; mild anemia
• C-reactive protein: Markedly elevated
• Erythrocyte sedimentation rate: Elevated
• Renal and liver function tests: Within normal limits
• HIV serology: Negative
• Hepatitis B and C serology: Positive for hepatitis C
Microbiological Evaluation:
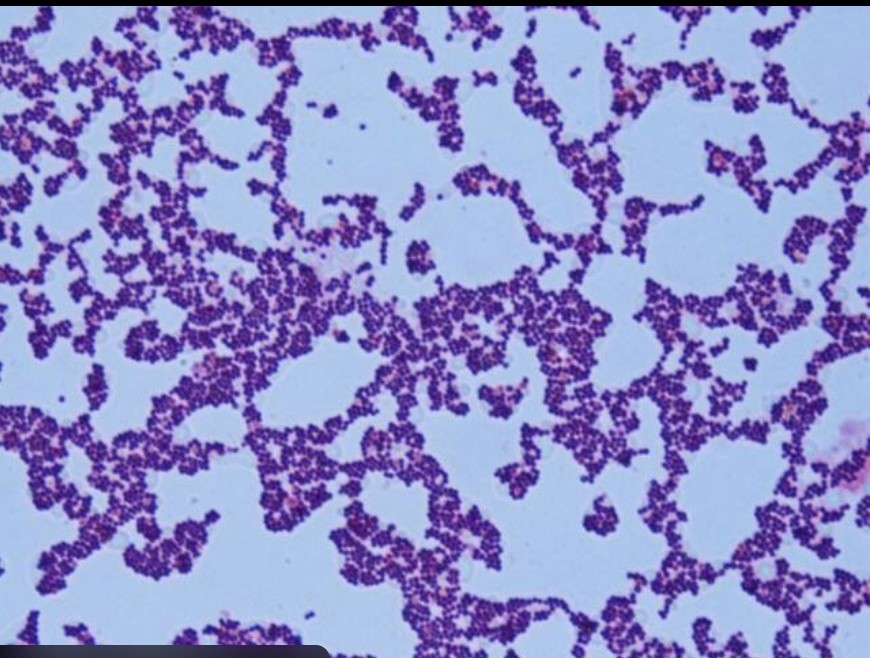
• Three sets of blood cultures obtained prior to antibiotic initiation
• Blood cultures grew methicillin-sensitive Staphylococcus aureus
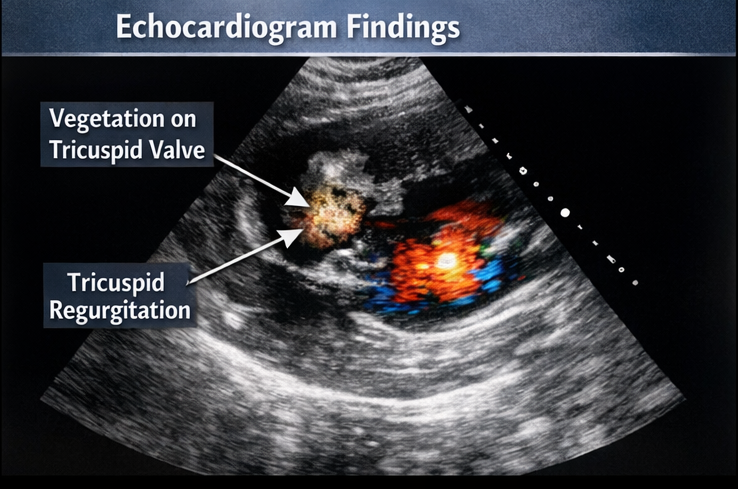
Echocardiographic Evaluation:
• Transthoracic echocardiography revealed a mobile vegetation measuring 1.5 cm on the tricuspid valve with moderate tricuspid regurgitation
• Left ventricular function was preserved
• No evidence of left-sided valve involvement
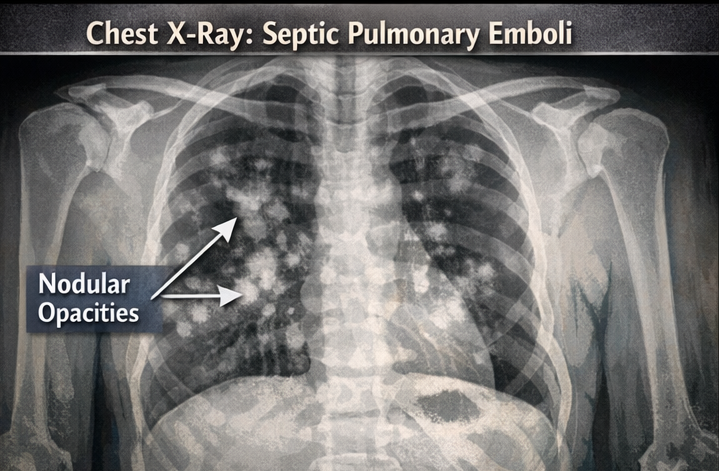
Radiological Evaluation:
• Chest X-ray showed multiple bilateral nodular opacities suggestive of septic pulmonary emboli. These findings fulfilled the modified Duke criteria for definite infective endocarditis.
Management and Outcome
Initial Management
The patient was admitted to the intensive care unit for close monitoring. Empirical intravenous antibiotic therapy was initiated after blood cultures were drawn.
Following culture and sensitivity results, antibiotics were tailored to intravenous cloxacillin. Supportive care included antipyretics, intravenous fluids, and oxygen therapy as needed.
Ongoing Management
• Serial blood cultures were monitored to ensure clearance of bacteremia
• Daily clinical assessments for signs of heart failure or embolic complications
• Addiction medicine consultation was obtained for substance use counseling
• Hepatology consultation was arranged for hepatitis C management
Surgical intervention was not immediately indicated, as the patient remained hemodynamically stable with no evidence of refractory infection or severe valve dysfunction.
Follow-Up and Outcome
The patient became afebrile by day five of targeted antibiotic therapy. Repeat blood cultures obtained after 72 hours of treatment were sterile. Inflammatory markers showed a gradual decline.
After two weeks, repeat echocardiography demonstrated a reduction in vegetation size with stable valve function. The patient completed a total of six weeks of intravenous antibiotic therapy under inpatient supervision.
At discharge, the patient was clinically stable with resolution of symptoms. He was enrolled in a substance use rehabilitation program and scheduled for cardiology and infectious disease follow-up.
Discussion
Infective endocarditis among IV drug users represents a distinct clinical entity with unique epidemiological and clinical features. Staphylococcus aureus is the predominant pathogen, and right-sided valve involvement is common due to direct inoculation of pathogens into the venous circulation.
Diagnosis can be challenging due to overlapping symptoms with other infectious conditions. Blood cultures and echocardiography remain central to diagnosis, while imaging studies assist in identifying complications such as septic emboli.
Medical management with prolonged intravenous antibiotics is effective in most cases. Surgical intervention is reserved for patients with persistent bacteremia, large vegetations with recurrent emboli, severe valve dysfunction, or heart failure.
This case underscores the importance of early recognition, targeted antimicrobial therapy, and addressing underlying substance use to prevent recurrence and improve long-term outcomes.
Conclusion
Acute infective endocarditis is a serious complication of intravenous drug use and requires prompt diagnosis and aggressive management. Persistent fever in IV drug users should raise suspicion for IE, especially in the presence of cardiac murmurs or embolic phenomena. Early initiation of appropriate antibiotics, close monitoring for complications, and a multidisciplinary approach addressing both infection and substance use are essential for optimal patient outcomes.
References
- World Health Organization. (2023). Global report on infectious diseases and substance use. https://www.who.int
- Habib, G., Lancellotti, P., Antunes, M. J., et al. (2015). 2015 ESC guidelines for the management of infective endocarditis. European Heart Journal, 36(44), 3075–3128 https://pubmed.ncbi.nlm.nih.gov/26320109/
- Baddour, L. M., Wilson, W. R., Bayer, A. S., et al. (2015). Infective endocarditis in adults: Diagnosis, antimicrobial therapy, and management. Circulation, 132(15), 1435–1486 https://pubmed.ncbi.nlm.nih.gov/26373316/
- Miro, J. M., del Rio, A., & Mestres, C. A. (2009). Infective endocarditis in intravenous drug abusers and HIV-1 infected patients. Infectious Disease Clinics of North America, 23(2), 273–295 https://pubmed.ncbi.nlm.nih.gov/19393911
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Inner Thoughts of Leonard Bernstein, the "Maestro".
2.
Mobile prostate cancer screening clinic can ID the disease in disadvantaged men
3.
No Survival Benefit Seen With Adjuvant Atezolizumab in TNBC
4.
Parents, teachers at Missouri school want answers after string of cancer diagnoses
5.
A promising medication could slow brain tumors in children.
1.
Future-Ready Cancer Screening: What Every Clinician Should Know in 2025
2.
Cancer Evolution and Therapeutic Resistance: Mechanisms, Clinical Insights, and Emerging Strategies
3.
Targeting Cancer Stem Cells in Solid Tumors: Mechanisms, Clinical Implications, and Therapeutic Advances
4.
Partial Gland Ablation in Prostate Cancer: Oncologic Outcomes in Intermediate-Risk Cases
5.
Generative AI for Adaptive Oncology Trial Design
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Management of 1st line ALK+ mNSCLC (CROWN TRIAL Update) - Part III
2.
Revolutionizing Treatment of ALK Rearranged NSCLC with Lorlatinib - Part I
3.
Recent Data Analysis for First-Line Treatment of ALK+ NSCLC
4.
INO-VATE: The Long-Term Overall Survival Analysis in Iontuzumab-Treated Patients
5.
Current Scenario of Cancer- The Incidence of Cancer in Men

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge