Cardiomegaly: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Cardiomegaly, defined as an enlargement of the heart, is a radiological and clinical finding rather than a disease entity itself. It reflects underlying cardiac pathology such as hypertensive heart disease, cardiomyopathy, valvular disorders, or ischemic heart disease. Patients may present with a spectrum ranging from asymptomatic findings on imaging to overt heart failure.
We report the case of a 52-year-old male presenting with progressive breathlessness and fatigue. Imaging studies revealed cardiomegaly, and further evaluation confirmed dilated cardiomyopathy secondary to long-standing uncontrolled hypertension. The patient was managed with guideline-directed medical therapy, resulting in significant symptomatic improvement.
This case emphasizes the importance of early detection, comprehensive evaluation, and targeted management of cardiomegaly to prevent progression to heart failure and improve clinical outcomes.
Introduction
Cardiomegaly refers to an abnormal increase in the size of the heart, typically identified through imaging modalities such as chest X-ray, echocardiography, or cardiac MRI. It is most commonly associated with conditions that impose chronic pressure or volume overload on the heart, leading to structural remodeling.
The condition may involve dilation of cardiac chambers, hypertrophy of myocardial walls, or a combination of both. While cardiomegaly itself may be asymptomatic, it often signifies underlying cardiovascular pathology that requires prompt diagnosis and management.
Globally, cardiomegaly is frequently associated with hypertension, coronary artery disease, and cardiomyopathies. In developing regions, additional etiologies such as rheumatic heart disease and infectious causes also contribute significantly.
Early recognition is essential, as untreated cardiomegaly can progress to heart failure, arrhythmias, thromboembolic events, and sudden cardiac death.
Case Report
Patient History
A 52-year-old male presented to the outpatient department with:
- Progressive shortness of breath over 6 months
- Easy fatigability
- Occasional palpitations
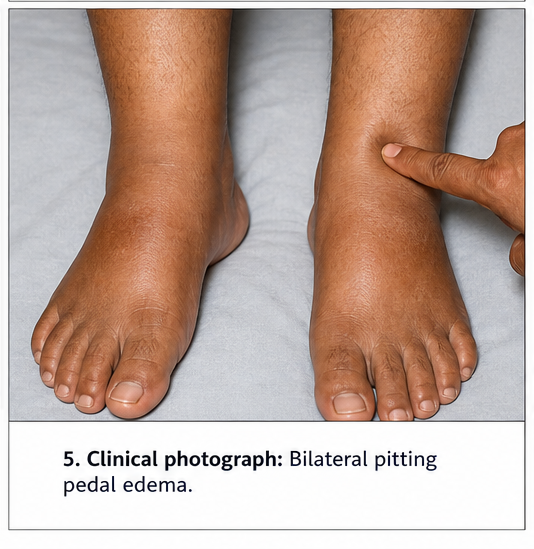
- Mild bilateral lower limb swelling
There was no history of chest pain, syncope, or fever. The patient had a known history of hypertension for 10 years but reported poor compliance with medications. There was no history of diabetes, smoking, or alcohol abuse.
Family history was unremarkable for cardiovascular disease.
Clinical Examination
General Examination
- Patient conscious and oriented
- Blood pressure: 160/100 mmHg
- Pulse: 96 beats per minute, regular
- Respiratory rate: 20 breaths per minute
- Mild pedal edema present
Cardiovascular Examination
- Apex beat displaced laterally (6th intercostal space, anterior axillary line)
- Diffuse and sustained apical impulse
- Presence of S3 gallop
- No significant murmurs
Respiratory Examination
- Bilateral basal crepitations
Abdominal Examination
- Mild hepatomegaly
Clinical Evaluation
Differential Diagnosis
Based on clinical findings, the following were considered:
- Dilated cardiomyopathy
- Hypertensive heart disease
- Ischemic cardiomyopathy
- Valvular heart disease
- Pericardial effusion
The presence of long-standing hypertension and displaced apex beat suggested a structural cardiac abnormality.
Investigations
Laboratory Tests
- Complete blood count: Within normal limits
- Renal function tests: Mildly elevated creatinine
- Liver function tests: Mild elevation in liver enzymes
- BNP (B-type natriuretic peptide): Elevated
- Thyroid profile: Normal
Imaging
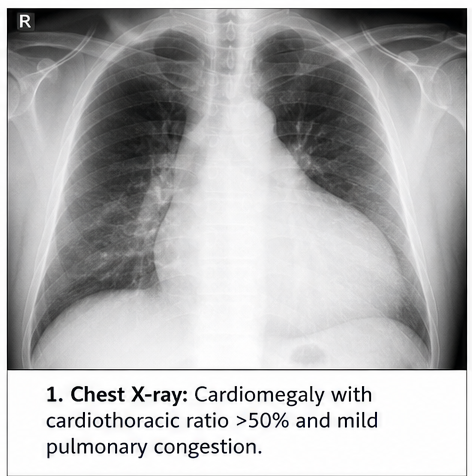
Chest X-ray
- Enlarged cardiac silhouette
- Cardiothoracic ratio >50%
- Mild pulmonary congestion
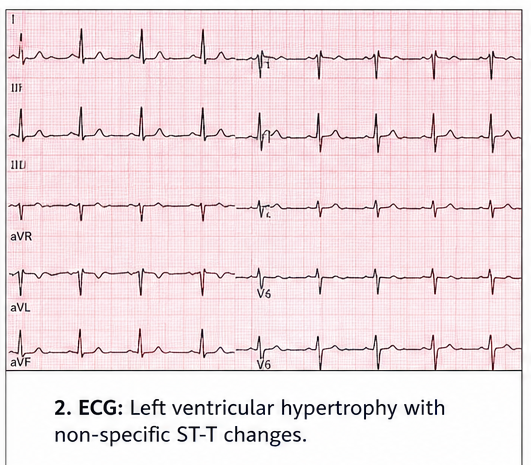
Electrocardiogram (ECG)
- Left ventricular hypertrophy
- Non-specific ST-T changes
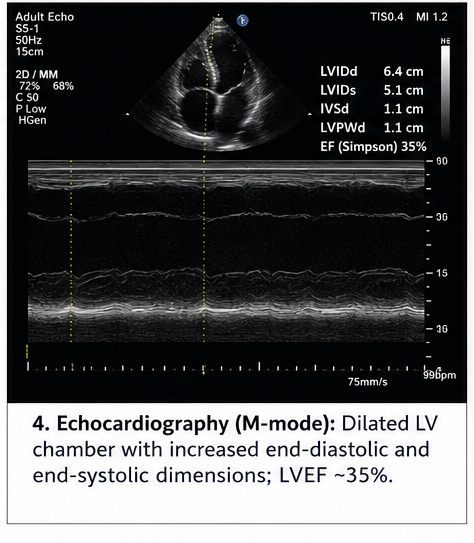
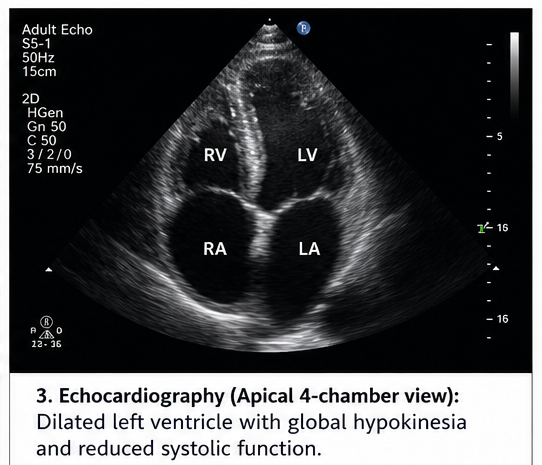
Echocardiography
- Dilated left ventricle
- Reduced ejection fraction (~35%)
- Global hypokinesia
- Mild mitral regurgitation
Cardiac MRI (if performed)
- Confirmed dilated cardiomyopathy
- No evidence of infiltrative disease
Diagnosis
A diagnosis of cardiomegaly secondary to dilated cardiomyopathy due to uncontrolled hypertension was established based on clinical findings, imaging, and functional assessment.
Management and Outcome
Management Strategy
The treatment approach focused on:
- Symptom control
- Improvement of cardiac function
- Prevention of complications
- Management of underlying hypertension
Medical Management
- ACE inhibitors (for afterload reduction)
- Beta-blockers (for heart rate control and remodeling)
- Diuretics (for fluid overload)
- Aldosterone antagonists
- Lifestyle modifications including salt restriction and weight control
Supportive Measures
- Fluid restriction
- Regular blood pressure monitoring
- Patient education on medication adherence
Clinical Course
During hospitalization:
- Symptomatic improvement in breathlessness
- Reduction in edema
- Stabilization of blood pressure
Follow-Up
At 2 Weeks
- Improved exercise tolerance
- Reduced pedal edema
At 1 Month
- Stable vitals
- Improved functional status
At 6 Months
- Ejection fraction improved to 45%
- No hospital readmissions
- Good compliance with therapy
Discussion
Pathophysiology
Cardiomegaly results from adaptive and maladaptive changes in the myocardium due to chronic hemodynamic stress. These include:
- Pressure overload (e.g., hypertension) → concentric hypertrophy
- Volume overload (e.g., valvular regurgitation) → chamber dilation
Over time, these changes lead to:
- Reduced contractility
- Ventricular remodeling
- Neurohormonal activation
This progression ultimately culminates in heart failure if untreated.
Etiology
Common causes of cardiomegaly include:
- Hypertension
- Coronary artery disease
- Cardiomyopathies (dilated, hypertrophic, restrictive)
- Valvular heart disease
- Congenital heart defects
- Pericardial diseases
In this case, uncontrolled hypertension was the primary contributing factor.
Epidemiology
- More common in middle-aged and elderly individuals
- Higher prevalence in patients with chronic hypertension
- Increasing incidence due to lifestyle-related risk factors
Clinical Manifestations
Early Stage
- Often asymptomatic
- Incidental finding on imaging
Progressive Stage
- Dyspnea
- Fatigue
- Palpitations
- Edema
Advanced Stage
- Heart failure symptoms
- Arrhythmias
- Syncope
Diagnostic Considerations
A systematic approach is essential:
- Clinical evaluation
- Imaging (Chest X-ray, Echocardiography)
- Functional assessment (ejection fraction)
- Identification of underlying cause
Echocardiography remains the cornerstone for diagnosis and evaluation of cardiac function.
Treatment Considerations
Management depends on the underlying cause and severity.
Medical Therapy
- First-line treatment in most cases
- Focuses on reversing remodeling and improving function
Device Therapy
- Implantable cardioverter-defibrillator (ICD) in selected cases
- Cardiac resynchronization therapy (CRT)
Surgical Options
- Valve repair or replacement
- Coronary artery bypass grafting (if ischemic cause)
Complications
If untreated, cardiomegaly can lead to:
- Heart failure
- Arrhythmias
- Thromboembolism
- Sudden cardiac death
Prognosis
The prognosis depends on:
- Underlying etiology
- Degree of cardiac dysfunction
- Timeliness of intervention
- Patient compliance
With appropriate management, many patients experience significant improvement in quality of life.
Conclusion
Cardiomegaly is a significant clinical finding that often reflects underlying cardiovascular pathology. This case underscores the importance of early diagnosis, especially in patients with risk factors such as hypertension.
A structured approach involving clinical evaluation, imaging, and functional assessment is essential for accurate diagnosis. Timely initiation of guideline-directed medical therapy can significantly improve outcomes and prevent disease progression.
While cardiomegaly may initially present as a silent condition, its potential complications necessitate vigilant monitoring and long-term management. Patient education, adherence to therapy, and regular follow-up play a critical role in optimizing clinical outcomes.
A comprehensive, individualized treatment strategy ensures not only symptom relief but also improved survival and quality of life for affected patients.
References
- Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med. https://pubmed.ncbi.nlm.nih.gov/2934510/
- McMurray JJV, Adamopoulos S, Anker SD, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. https://pubmed.ncbi.nlm.nih.gov/20805041/
- Yancy CW, Jessup M, Bozkurt B, et al. ACC/AHA guideline for the management of heart failure. J Am Coll Cardiol. https://pubmed.ncbi.nlm.nih.gov/23747642/
- StatPearls. Cardiomegaly – Clinical Overview and Management. https://www.ncbi.nlm.nih.gov/books/NBK542296/
- Braunwald E. Heart Disease: A Textbook of Cardiovascular Medicine. https://www.sciencedirect.com/book/9780323463423/braunwalds-heart-disease
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge