Actinomycetoma Presenting as Painless Nodules with Purulent Discharge: A Case Report
OthersPage Navigation
Abstract
Actinomycetoma is a chronic, progressive subcutaneous infection characterized by tumefaction, sinus tract formation, and purulent discharge containing granules [1]. We report a case of actinomycetoma caused by Nocardia brasiliensis in a middle-aged patient who presented with painless nodular swellings and intermittent pus discharge. Early clinical suspicion, supported by characteristic cutaneous findings and microbiological confirmation, enabled prompt initiation of therapy, preventing deeper tissue and bone involvement [2]. This case highlights the importance of recognizing early dermatological features of actinomycetoma to reduce morbidity.
Introduction
Mycetoma is a chronic granulomatous infection of the skin and subcutaneous tissues, commonly affecting individuals in tropical and subtropical regions, particularly those engaged in agricultural or outdoor occupations with frequent exposure to soil and plant matter [1]. The disease is endemic in areas known as the “mycetoma belt,” which includes parts of Africa, Latin America, and South Asia. Infection is usually acquired through traumatic inoculation of the causative organism into the skin, often through minor cuts or puncture wounds that may go unnoticed by the patient [1].
Based on the etiological agent, mycetoma is broadly classified into eumycetoma, caused by true fungi, and actinomycetoma, caused by aerobic filamentous bacteria. Actinomycetoma is most commonly attributed to Nocardia species, particularly Nocardia brasiliensis, and is recognized for its relatively aggressive local invasion and faster progression compared to eumycetoma [2]. Without timely intervention, actinomycetoma can extend into deeper soft tissues and underlying bone, leading to deformity, functional impairment, and chronic disability.
.png)
Clinically, the disease typically presents with a triad of painless subcutaneous swelling, sinus tract formation, and purulent discharge that may contain characteristic granules [3]. The absence of significant pain and systemic symptoms often contributes to delayed diagnosis, allowing the infection to progress insidiously over months or years. Such delays increase the risk of complications and complicate management, underscoring the importance of early recognition and prompt treatment to improve outcomes [2,3].
Case Report
Patient History
A 42-year-old male agricultural worker presented with multiple painless swellings over the lower limb of 8 months’ duration [1]. The lesions had gradually increased in both number and size and were associated with intermittent purulent discharge from multiple sinus openings. The discharge was occasionally noted to contain fine granular material, a characteristic feature suggestive of mycetoma [1]. There was no associated pain, erythema, or local warmth over the affected area. The patient denied any history of fever, weight loss, or other systemic symptoms, which is consistent with the indolent nature of actinomycetoma [2].

He did not recall any specific episode of trauma; however, his occupation involved prolonged and repeated exposure to soil and organic matter, often while working barefoot or with minimal protective footwear. Such occupational exposure is a well-established risk factor for actinomycetoma, as traumatic inoculation of the causative organism from soil is the primary mode of transmission [1,2]. There was no history of diabetes mellitus, immunosuppression, or prior similar lesions, and no family history of chronic granulomatous infections.
On clinical examination, the swellings were firm to soft in consistency, non-tender, and localized to the subcutaneous tissue without limitation of joint movements. The overlying skin showed multiple active and healed sinus tracts with surrounding induration. Regional lymphadenopathy was absent, and systemic examination was unremarkable [2]. Routine laboratory investigations were within normal limits, with no evidence of systemic infection.
Based on the chronic course, painless nodules, draining sinuses with purulent discharge, and significant occupational soil exposure, a provisional diagnosis of actinomycetoma was made [1–3]. Further microbiological and histopathological evaluation was planned to confirm the diagnosis and differentiate it from eumycetoma and other chronic subcutaneous infections, enabling timely initiation of appropriate therapy and prevention of deep tissue or bone involvement [2,3].
Clinical Findings
Cutaneous examination revealed multiple firm to soft subcutaneous nodules clustered over the affected limb, predominantly involving the lower extremity [1]. The nodules varied in size and were irregularly distributed, with some appearing coalescent, giving rise to localized swelling of the affected area. Several nodules demonstrated well-formed sinus openings with active purulent discharge, occasionally containing fine granular material, which is characteristic of mycetoma and supports the clinical diagnosis [2]. The surrounding skin showed mild induration, likely reflecting chronic inflammation, but remained non-tender, with no associated erythema, warmth, or signs of acute infection.


The absence of pain and minimal inflammatory changes on the skin surface were notable and are typical features of actinomycetoma, contributing to its often delayed diagnosis [1,2]. There was no evidence of ulceration, necrosis, or secondary bacterial infection. Palpation did not elicit tenderness, and the underlying muscles appeared uninvolved on clinical assessment. Joint mobility of the adjacent joints was preserved, with no restriction of movement or functional limitation at the time of presentation.
No regional lymphadenopathy was detected, which is consistent with the localized nature of actinomycetoma and its tendency to spread contiguously rather than via lymphatic routes [2,3]. Systemic examination was unremarkable, and there were no clinical signs suggestive of disseminated disease. Taken together, the presence of painless subcutaneous swelling, multiple draining sinuses, and chronic indurated skin changes were in keeping with the classical clinical triad of actinomycetoma [2]. These characteristic findings, when correlated with the patient’s occupational exposure and chronic disease course, strongly supported the provisional diagnosis and emphasized the need for confirmatory microbiological and histopathological evaluation to guide appropriate management [1–3].
Investigations
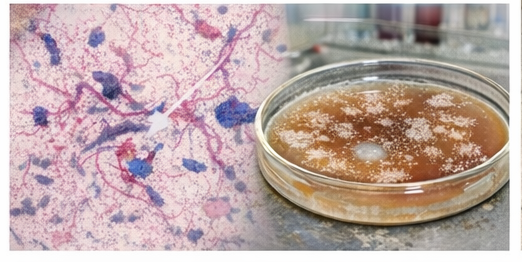
Microscopic examination of the purulent discharge demonstrated filamentous, branching organisms. Gram staining showed gram-positive filaments, and modified acid-fast staining supported Nocardia species [3]. Culture confirmed Nocardia brasiliensis, the most frequently implicated organism in actinomycetoma [2]. Radiographic imaging showed no evidence of bone involvement, indicating early-stage disease.
Discussion
Actinomycetoma typically presents with painless subcutaneous nodules that gradually enlarge and coalesce, eventually leading to the formation of multiple draining sinuses that discharge purulent material containing characteristic granules [1,4]. These granules represent colonies of the causative organism and may vary in color and consistency, providing important diagnostic clues for clinicians and microbiologists alike [5]. The lesions most commonly involve the feet, lower limbs, and other exposed areas of the body, reflecting the role of traumatic inoculation from contaminated soil or plant material [1,6]. The absence of pain, fever, or other systemic symptoms frequently results in delayed medical consultation, allowing the disease to progress unnoticed over extended periods and increasing the risk of complications [4,5].
Among the causative organisms, Nocardia brasiliensis accounts for a large proportion of actinomycetoma cases worldwide and is particularly prevalent in tropical and subtropical regions [2,6]. Infections caused by Nocardia species are associated with relatively rapid tissue destruction and a higher propensity for local spread compared with fungal mycetoma if left untreated [2,4]. Progressive involvement of deeper soft tissues and underlying bone can lead to chronic osteomyelitis, deformity, secondary bacterial infection, and significant functional impairment [2,5].
Accurate differentiation between actinomycetoma and eumycetoma is therefore critical, as treatment strategies, duration of therapy, and prognoses differ substantially [3,4]. Actinomycetoma generally responds well to prolonged, targeted antibiotic therapy, often administered in combination regimens over several months, whereas eumycetoma typically shows limited response to medical therapy alone and frequently requires surgical excision or even amputation in advanced cases [3,5,6]. Early diagnosis and timely initiation of appropriate antimicrobial treatment, as demonstrated in this case, can halt disease progression, preserve anatomical structures, and prevent long-term morbidity and disability [1–6].
Conclusion
Actinomycetoma should be strongly considered in patients presenting with painless subcutaneous nodules accompanied by purulent discharge, especially in individuals with a history of occupational or environmental exposure to soil, such as agricultural workers, laborers, and those residing in endemic tropical and subtropical regions [1]. The chronic, indolent nature of the disease often leads to underrecognition in its early stages, as patients may not perceive the lesions as serious due to the absence of pain or systemic symptoms. As a result, delayed presentation is common, increasing the risk of progressive local invasion.
Early clinical suspicion, supported by appropriate diagnostic investigations such as microbiological culture, histopathological examination, and imaging studies, is essential for accurate diagnosis and timely initiation of therapy [1,2]. Identification of the causative organism not only confirms the diagnosis but also guides the selection of effective antimicrobial regimens, which are critical for successful disease control in actinomycetoma. Imaging modalities, including radiography or magnetic resonance imaging, can help assess the extent of soft tissue and bone involvement and serve as a baseline for monitoring treatment response [2].
Prompt and adequate treatment can halt disease progression and prevent extension into deeper tissues and underlying bone, thereby reducing the risk of chronic osteomyelitis, deformity, and functional disability [2,3]. Early intervention also minimizes the need for surgical procedures, preserves limb function, and improves overall quality of life. This underscores the importance of clinician awareness and early referral in suspected cases, as timely diagnosis and appropriate management remain key determinants of favorable long-term outcomes in actinomycetoma [1,2,3].
References
- Zijlstra EE, van de Sande WWJ, Welsh O, et al. Mycetoma: A unique neglected tropical disease. PLoS Neglected Tropical Diseases.
- Welsh O, Al-Abdely HM, Salinas-Carmona MC, Fahal AH. Mycetoma medical therapy. PLoS Negl Trop Dis.
- Bonifaz A, Tirado-Sánchez A, Calderón L, et al. Mycetoma: Experience of 482 cases in a single center in Mexico. PLoS Negl Trop Dis.
- Fahal AH. Mycetoma: A global medical and socio-economic dilemma. PLoS Neglected Tropical Diseases. 2017;11(4):e0005509.
- van de Sande WWJ. Global burden of human mycetoma: A systematic review and meta-analysis. PLoS Neglected Tropical Diseases. 2013;7(11):e2550.
- Fahal AH, Suliman SH, Hay R. Mycetoma: The spectrum of clinical presentation.
Tropical Medicine & International Health. 2018;23(1):105–112.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Does pollution cause cancer?
2.
AI is equally capable of reading breast cancer scans as human radiologists.
3.
EVP Beats Cisplatin for Resectable MIBC
4.
New research points out a promising strategy for treating metastatic medulloblastoma
5.
Academics + Pharma = Big Bucks; New CAR-T Warnings; Patients Seek Cancer Tests.
1.
A Closer Look at Breast Cancer: Examining the Ultrasound Images
2.
Unlocking the Secrets of Oral Cancer Staging: A New Approach to Early Detection
3.
Impact of Hormone Therapy Cessation on Tumor Growth: Case Study of Ki-67 Reduction
4.
Unraveling the Mysteries of Lymphoma: A Journey into the Unknown
5.
Refining AML Survival: Prognostic Factors, Therapies, and Stem Cell Strategies Reviewed
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Navigating the Complexities of Ph Negative ALL - Part III
2.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VIII
3.
Management of 1st line ALK+ mNSCLC (CROWN TRIAL Update)
4.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part III
5.
Virtual Case Study on Pedal Edema and Triple Vessel Disease - An Initiative by Hidoc Dr.

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge