Pancreatic Calcification: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Pancreatic calcification is a characteristic feature of chronic pancreatitis, representing long-standing inflammation and irreversible structural damage to the pancreatic parenchyma. It is commonly associated with alcohol abuse, metabolic abnormalities, or idiopathic etiologies. Patients typically present with chronic abdominal pain, malabsorption, steatorrhea, and endocrine dysfunction such as diabetes mellitus. Radiological imaging, particularly contrast-enhanced computed tomography (CT), plays a pivotal role in diagnosis by demonstrating intraductal and parenchymal calcifications.
This case report describes a 45-year-old male presenting with recurrent abdominal pain and weight loss, ultimately diagnosed with chronic calcific pancreatitis. The report emphasizes the diagnostic approach, therapeutic management, and favorable clinical outcome following timely intervention and lifestyle modification.
Introduction
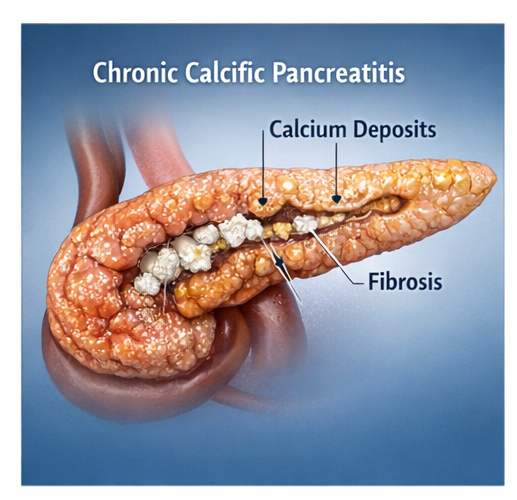
Pancreatic calcification is most frequently seen in the setting of chronic pancreatitis, a progressive inflammatory disease characterized by fibrosis, ductal distortion, and eventual loss of both exocrine and endocrine pancreatic function. The formation of calcifications results from precipitation of calcium salts within proteinaceous plugs in the pancreatic ducts, leading to obstruction and further glandular damage.
The global burden of chronic pancreatitis is significant, particularly in regions with high alcohol consumption and tropical pancreatitis prevalence. The disease is associated with substantial morbidity, including chronic pain syndromes, malnutrition, and diabetes.
Risk factors include chronic alcohol intake, smoking, genetic mutations, autoimmune processes, and metabolic disturbances such as hypercalcemia and hypertriglyceridemia. Early recognition and appropriate management are crucial to prevent complications and improve patient outcomes.
Case Report
Patient History
A 45-year-old male presented to the gastroenterology outpatient department with complaints of recurrent upper abdominal pain for the past 8 months.
The pain was dull, aching, and localized to the epigastric region, with radiation to the back. It was aggravated after meals and partially relieved by leaning forward.
The patient also reported:
-
Progressive weight loss (~7 kg over 6 months)
-
Decreased appetite
-
Intermittent nausea
-
Passage of bulky, foul-smelling, oily stools suggestive of steatorrhea
There was a significant history of chronic alcohol consumption (approximately 60–80 g/day) for over 15 years. There was no history of gallstone disease, prior abdominal surgery, or known metabolic disorders.
Clinical Examination
On examination:
-
Mild epigastric tenderness was noted
-
No palpable mass or organomegaly
-
No icterus or lymphadenopathy
Vital parameters were stable, and systemic examination was unremarkable.
Clinical Evaluation
Differential Diagnosis
Based on clinical presentation, the following conditions were considered:
-
Chronic pancreatitis
-
Pancreatic carcinoma
-
Peptic ulcer disease
-
Gallstone-related pancreatitis
-
Functional dyspepsia
The chronicity of symptoms, steatorrhea, and alcohol history strongly suggested chronic pancreatitis.
Investigations
Laboratory Findings
-
Serum amylase and lipase: Mildly elevated
-
Fasting blood glucose: Elevated (indicative of impaired glucose metabolism)
-
Liver function tests: Within normal limits
-
Serum calcium and triglycerides: Normal
Imaging Studies
Ultrasound Abdomen:
-
Irregular, heterogeneous pancreatic echotexture
-
Multiple echogenic foci with acoustic shadowing
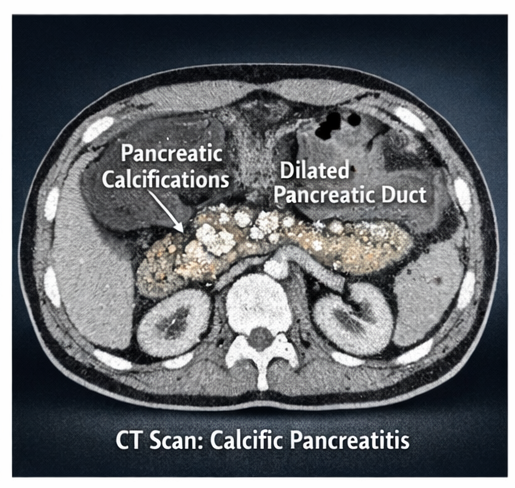
Contrast-Enhanced CT Scan (CECT):
-
Multiple calcifications within the pancreatic duct and parenchyma
-
Dilatation of the main pancreatic duct
-
Pancreatic atrophy
These findings were diagnostic of chronic calcific pancreatitis.
Diagnosis
Based on clinical presentation and radiological confirmation, the diagnosis was established as:
Chronic calcific pancreatitis with exocrine and early endocrine insufficiency secondary to chronic alcohol use
Management and Outcome
Initial Management
The patient was managed conservatively with a multidisciplinary approach involving gastroenterologists, dieticians, and endocrinologists.

Pharmacological Treatment
-
Pancreatic enzyme replacement therapy (PERT) to improve digestion
-
Analgesics following a stepwise approach for pain control
-
Proton pump inhibitors to enhance enzyme efficacy
-
Insulin therapy for glycemic control
Lifestyle and Dietary Modifications
-
Strict abstinence from alcohol
-
Low-fat, high-protein diet
-
Small, frequent meals

Supportive Measures
-
Nutritional supplementation
-
Fat-soluble vitamins (A, D, E, K)
-
Patient education regarding disease progression
Follow-Up
At 2 weeks:
-
Marked reduction in abdominal pain
-
Improved appetite
At 1 month:
-
Decrease in steatorrhea
-
Weight stabilization
At 3 months:
-
Significant symptomatic improvement
-
Better glycemic control
-
Improved quality of life
Outcome
The patient demonstrated:
-
Effective pain relief
-
Improved nutritional status
-
Stabilization of pancreatic function
-
No recurrence of acute exacerbations
Discussion
Pancreatic calcification is a hallmark of advanced chronic pancreatitis and signifies long-standing, irreversible damage to the pancreatic parenchyma, often reflecting the end stage of a progressive inflammatory process. It is associated with repeated episodes of pancreatic injury, leading to structural remodeling, fibrosis, and loss of both exocrine and endocrine function over time.
The pathogenesis involves the formation of intraductal protein plugs due to altered pancreatic secretions, particularly decreased bicarbonate and increased protein concentration. These plugs act as a nidus for calcium salt deposition, eventually resulting in calcified stones within the pancreatic ducts and parenchyma. Progressive calcification leads to ductal obstruction, increased intraductal pressure, and further parenchymal damage, perpetuating a cycle of inflammation and fibrosis that contributes to glandular atrophy and functional impairment.
Etiology and Risk Factors
Common causes include:
-
Chronic alcohol consumption
-
Idiopathic pancreatitis
-
Tropical pancreatitis
-
Genetic mutations (PRSS1, SPINK1)
-
Metabolic abnormalities
Clinical Features
Patients typically present with:
-
Chronic epigastric pain radiating to the back
-
Weight loss
-
Steatorrhea
-
Diabetes mellitus
Diagnostic Approach
-
Detailed clinical history
-
Laboratory investigations
-
Imaging (CT scan as gold standard)
-
Endoscopic evaluation (if indicated)
CT imaging remains the most sensitive modality for detecting pancreatic calcifications.
Management Strategies
1. Medical Management
-
Pain control
-
Enzyme supplementation
-
Glycemic management
2. Lifestyle Modification
-
Alcohol cessation
-
Dietary regulation
3. Interventional Management
-
Endoscopic therapy for ductal stones
-
Surgical decompression in refractory cases
Complications
If untreated, chronic pancreatitis with calcification may lead to:
-
Pancreatic pseudocysts
-
Diabetes mellitus
-
Severe malnutrition
-
Pancreatic malignancy
Prognosis
The prognosis depends on disease severity, adherence to treatment, and lifestyle modification. Early intervention and alcohol abstinence significantly improve outcomes, although structural damage is largely irreversible.
Conclusion
Pancreatic calcification is a critical indicator of chronic pancreatitis and signifies advanced disease with irreversible pancreatic damage. This case highlights the importance of early clinical suspicion in patients with chronic abdominal pain and relevant risk factors such as long-term alcohol use.
A systematic diagnostic approach, particularly the use of CT imaging, enables accurate identification of calcifications and disease severity. Timely initiation of enzyme replacement therapy, adequate pain management, and strict lifestyle modifications are essential in improving patient outcomes and preventing complications.
Preventive strategies, including alcohol cessation and nutritional optimization, play a pivotal role in disease control. With appropriate management and follow-up, patients can achieve significant symptomatic relief and improved quality of life despite the chronic nature of the disease.
References
-
Whitcomb DC. Chronic pancreatitis: an update on pathogenesis and management. https://pubmed.ncbi.nlm.nih.gov/
-
Yadav D, Lowenfels AB. Epidemiology of pancreatitis and pancreatic cancer. https://pubmed.ncbi.nlm.nih.gov/
-
Stevens T, Conwell DL. Chronic pancreatitis: diagnosis and management. https://pubmed.ncbi.nlm.nih.gov/
-
Drewes AM, et al. Pain management in chronic pancreatitis. https://pubmed.ncbi.nlm.nih.gov/
-
Braganza JM, et al. Chronic pancreatitis and calcification mechanisms. https://pubmed.ncbi.nlm.nih.gov/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Biomarker-Selected Treatment Shows Promise for Bladder Preservation in MIBC
2.
FDA Investigating Blood Cancer Risk With Gene Therapy Skysona
3.
Surviving cancer, still suffering: Survey reveals gaps in follow‑up care
4.
Charles III, King of Kings, is Cancerous.
5.
The Truth About Apple AirPods
1.
How Digital Innovation and AI-Powered Case Studies are Revolutionizing Oncology Education?
2.
Advancements in Survival Mechanisms and Prognostic Determinants in Acute Myeloid Leukemia
3.
Unveiling the Hidden Mechanisms of Hemolytic Reactions
4.
Blastic Plasmacytoid Dendritic Cell Neoplasm and the Dawn of AI-powered Diagnostics
5.
Understanding Epoetin and Its Role in Treating Chronic Kidney Disease
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Current Scenario of Cancer- Q&A Session to Close the Gap
2.
Molecular Contrast: EGFR Axon 19 vs. Exon 21 Mutations - Part V
3.
Updates on Standard V/S High Risk Myeloma Treatment- The Next Part
4.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
5.
Incidence of Lung Cancer- An Overview to Understand ALK Rearranged NSCLC

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge