Rhinophyma in a Middle-Aged Male: A Case Report
OthersPage Navigation
Abstract
Rhinophyma is a rare, progressive form of phymatous rosacea characterized by hypertrophy of the sebaceous glands and connective tissue of the nose, leading to cosmetic disfigurement and functional impairment [1]. It predominantly affects middle-aged to elderly men and represents the end stage of chronic rosacea. We report a case of rhinophyma in a 55-year-old male who presented with progressive nasal enlargement, nodularity, and skin thickening over several years. Clinical evaluation and histopathological findings confirmed the diagnosis. Surgical debulking resulted in satisfactory cosmetic and functional outcomes. This case emphasizes the importance of early recognition and timely intervention to prevent advanced deformity and psychosocial distress.
Introduction
Rhinophyma is a benign but disfiguring condition classified under phymatous rosacea, characterized by progressive hypertrophy of sebaceous glands, connective tissue proliferation, and vascular dilation of the nasal skin [1,2]. The term “rhinophyma” is derived from the Greek words rhinos (nose) and phyma (growth), reflecting the hallmark nasal enlargement seen in advanced disease [3].
Although rosacea affects both sexes, rhinophyma occurs almost exclusively in men, typically between the fifth and seventh decades of life, with a male-to-female ratio reported as high as 12:1 [2,4]. The exact pathogenesis remains incompletely understood, but chronic inflammation, sebaceous gland hyperplasia, vascular instability, and possible microbial factors such as Demodex folliculorum are believed to contribute to disease progression [3,5].
Clinically, rhinophyma presents with nasal bulbous enlargement, irregular nodularity, thickened skin, dilated pores, and telangiectasia. In advanced cases, nasal airway obstruction, secondary infection, and ulceration may occur [4]. The condition can lead to significant psychological distress, social stigma, and impaired quality of life. Early diagnosis and appropriate management are therefore essential to prevent progression and restore nasal contour and function [1,5].
Case Report
Patient History
A 55-year-old male presented to the dermatology clinic with progressive enlargement and deformity of the nose over the past 6 years. The patient initially noticed persistent facial redness and episodic flushing, followed by gradual thickening of the nasal skin. Over time, the nose became increasingly bulbous with irregular surface nodularity.

There was no history of pain, ulceration, or purulent discharge. The patient denied any nasal trauma or prior dermatological treatment. He reported mild nasal obstruction in recent months due to narrowing of the external nares. There were no systemic symptoms such as fever or weight loss. His medical history was unremarkable, with no history of alcoholism, despite common misconceptions historically associated with rhinophyma [2,6].
Clinical Findings
Cutaneous examination revealed diffuse enlargement of the nasal tip and alae with lobulated, nodular contours. The overlying skin was thickened, erythematous, and greasy, with prominent sebaceous openings and telangiectasia. Multiple irregular nodules were noted, giving the nose a distorted and bulbous appearance.
Palpation revealed firm but non-tender tissue without fluctuance or signs of secondary infection. The surrounding facial skin demonstrated features of rosacea, including centrofacial erythema and mild papulopustular lesions. No cervical lymphadenopathy was detected. Examination of the eyes and oral cavity was normal. These findings were consistent with advanced rhinophyma [1,3].
Investigations
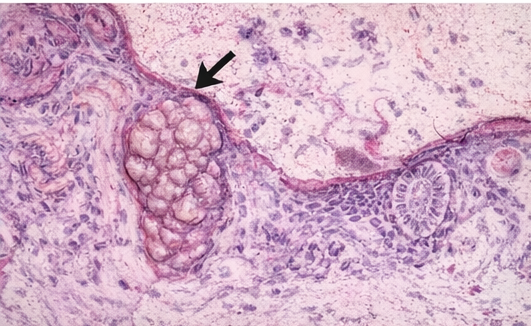
Routine laboratory investigations were within normal limits. A punch biopsy of the nasal skin was performed to exclude malignancy and confirm the diagnosis. Histopathological examination demonstrated marked sebaceous gland hyperplasia, dilated follicular infundibula filled with keratinous material, dermal fibrosis, and chronic inflammatory infiltrate, consistent with rhinophyma [4,5].
No evidence of basal cell carcinoma or squamous cell carcinoma was identified. Imaging was not required as there was no suspicion of deep tissue invasion.


Management and Outcome
The patient underwent surgical debulking using tangential excision combined with electrosurgical contouring under local anesthesia. Excess hypertrophic tissue was removed, preserving the underlying cartilage framework. Hemostasis was achieved, and the wound was allowed to heal by secondary intention.
Postoperative healing was uneventful, with significant improvement in nasal contour and airway patency. At 6-month follow-up, the patient reported marked improvement in self-esteem and social interactions, with no evidence of recurrence. Adjunctive medical management with topical metronidazole was initiated to control underlying rosacea and reduce the risk of progression [2,6].
Discussion
Rhinophyma represents the most severe manifestation of rosacea and is characterized by progressive tissue hypertrophy resulting in nasal disfigurement [1,4]. The disease typically evolves slowly over several years and is often preceded by long-standing, untreated, or inadequately controlled rosacea, particularly the erythematotelangiectatic and papulopustular subtypes. Chronic inflammation, vascular instability, sebaceous gland hyperplasia, and dermal fibrosis collectively contribute to the gradual enlargement and distortion of nasal contours. Despite its benign nature, rhinophyma can cause significant functional and psychological morbidity, including nasal airway obstruction, impaired breathing, social embarrassment, reduced self-esteem, and diminished quality of life [3,6]. The conspicuous facial involvement often leads to delayed presentation due to stigma or misconceptions regarding its etiology.
The differential diagnosis of rhinophyma includes sebaceous hyperplasia, benign and malignant nasal tumors, lupus pernio associated with sarcoidosis, granulomatous infections, and other causes of nasal skin thickening. Histopathological evaluation is therefore essential, not only to confirm the diagnosis but also to exclude coexisting malignancy. Importantly, basal cell carcinoma, squamous cell carcinoma, and other cutaneous neoplasms have been reported within rhinophymatous tissue in up to 5–10% of cases, underscoring the need for tissue sampling in suspicious or atypical lesions [5,7].
Medical therapy alone is generally ineffective in established rhinophyma, as irreversible tissue hypertrophy and fibrosis predominate in advanced disease. While systemic isotretinoin and topical agents may have a limited role in early phymatous changes, surgical modalities remain the mainstay of treatment in well-established cases [1,4,6]. Techniques such as scalpel excision, electrosurgery, laser ablation, and dermabrasion allow precise tissue debulking and contour restoration, often resulting in excellent cosmetic and functional outcomes. Early surgical intervention can prevent advanced deformity, minimize psychological distress, and reduce the need for extensive reconstructive procedures [1,6].
Conclusion
Rhinophyma is a chronic, progressive condition that predominantly affects middle-aged and elderly men and represents an advanced stage of rosacea [1,2]. Although benign in nature, it can result in marked cosmetic disfigurement, nasal obstruction, and considerable psychosocial distress, significantly impairing a patient’s quality of life [3,4]. The characteristic bulbous enlargement and nodularity of the nose often attract social stigma, which may lead to reduced self-esteem, social withdrawal, anxiety, and depressive symptoms [4,5]. Functional complications such as narrowing of the external nasal valves and impaired airflow may further exacerbate patient discomfort and contribute to delayed presentation [3,6].
Early recognition of rosacea and timely, appropriate management are essential to prevent progression to rhinophyma [1,2]. Identification and treatment of underlying inflammatory rosacea with medical therapies, including topical and systemic agents, may help control disease activity and slow phymatous changes in susceptible individuals [2,5]. Regular follow-up and patient counseling regarding trigger avoidance, skincare, and adherence to therapy play a crucial role in long-term disease control [5,6]. However, once established, rhinophyma is largely unresponsive to medical treatment alone, highlighting the importance of early intervention before irreversible sebaceous gland hyperplasia and dermal fibrosis develop [3,4].
In advanced cases, surgical intervention remains the treatment of choice and offers substantial improvement in both appearance and nasal function [1,4,6]. A variety of surgical techniques including scalpel excision, electrosurgery, laser resurfacing, and dermabrasion, can be tailored to disease severity and patient-specific factors, often yielding excellent cosmetic outcomes with low recurrence rates [4,6,7]. Increased clinician awareness, prompt referral, and comprehensive patient education are therefore critical to ensure early diagnosis, appropriate management, and optimal functional and psychosocial outcomes in individuals affected by rhinophyma [1–7].
References
- Lazzeri D, Colizzi L, Licata G, et al. Rhinophyma: Pathogenesis, diagnosis, and treatment. Journal of Plastic, Reconstructive & Aesthetic Surgery. 2012;65(4):437–444.
- Gallo RL, Granstein RD, Kang S, et al. Standard classification and pathophysiology of rosacea. Journal of the American Academy of Dermatology. 2018;78(1):148–155.
- Plewig G, Jansen T. Rosacea and rhinophyma: Clinical spectrum and pathogenesis. Journal of the European Academy of Dermatology and Venereology. 2009;23(6):629–639.
- Webster GF. Rosacea and rhinophyma. Dermatologic Clinics. 2018;36(2):139–150.
- Wollina U. Rhinophyma—A challenge for dermatologists and surgeons. Clinical, Cosmetic and Investigational Dermatology. 2019;12:365–372.
- Two AM, Wu W, Gallo RL, Hata TR. Rosacea: Part I. Introduction, classification, and pathophysiology. Journal of the American Academy of Dermatology. 2015;72(5):749–758.
- Powell FC. Clinical practice: Rosacea. New England Journal of Medicine. 2005;352(8):793–803.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Nuclear missile workers are contracting cancer: They blame the bases
2.
Mixed Results With Cyclophosphamide in Mismatched Unrelated Stem Cell Transplants
3.
New analysis helps discern benign from malignant thyroid growths
4.
MCh in Gynecologic Oncology: Admission, Medical School, Fees, Qualifications Information
5.
Even a few mutated cells can significantly impact how blood cancers develop, study finds
1.
Uncovering the Hidden Signs: How to Recognize the Early Symptoms of Colon Cancer
2.
The benefits and risks of taking fludrocortisone for adrenal insufficiency
3.
IGSF8: A Rising Star in Cancer Immunotherapy - Harnessing the Innate Immune System
4.
Innovative Intraoperative Therapies in Neurosurgical Oncology: Advancing Precision and Outcomes
5.
Different Types of Blood Dyscrasias
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
An In-Depth Look At The Signs And Symptoms Of Lymphoma
2.
Iron Deficiency Anemia: Ferric Maltol As a New Treatment Option- Further Discussion on A New Perspective
3.
Revolutionizing Treatment of ALK Rearranged NSCLC with Lorlatinib - Part VII
4.
Virtual Case Study on Pedal Edema and Triple Vessel Disease - An Initiative by Hidoc Dr.
5.
Nimotozumab Plus Chemo-radiotherapy v/s Placebo Plus Chemo-radiotherapy in Locally Advanced Nasopharyngeal Carcinoma

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge