Extramedullary Erythropoiesis: Clinical Evaluation, Multidisciplinary Management, and Outcome - A Case Report
OthersPage Navigation
Abstract
Extramedullary erythropoiesis (EME) is a compensatory hematopoietic phenomenon characterized by red blood cell production outside the bone marrow, typically occurring in response to chronic anemia, ineffective erythropoiesis, or bone marrow dysfunction. While commonly involving the liver and spleen, extramedullary hematopoietic tissue may rarely develop in atypical sites such as the skull, paranasal sinuses, and nasopharyngeal region. Pediatric presentations are uncommon and may mimic infectious, inflammatory, or neoplastic conditions, leading to diagnostic uncertainty.
We report a rare case of extramedullary erythropoiesis in a 3-year-old child presenting with sudden-onset fever and adenoid hypertrophy, with characteristic skull radiographic findings. This case highlights the importance of maintaining a high index of suspicion in anemic children with atypical radiological features, the role of imaging in diagnosis, and the value of a multidisciplinary approach in management and follow-up.
Introduction
Extramedullary erythropoiesis refers to the formation of erythroid precursor cells outside the medullary cavity of bones and represents a physiological compensatory response to chronic anemia or bone marrow insufficiency. It is most commonly associated with hemoglobinopathies such as thalassemia, sickle cell disease, congenital dyserythropoietic anemia, and myeloproliferative disorders [1].
In children, extramedullary erythropoiesis is relatively rare and often underrecognized, particularly when it involves uncommon anatomical locations. Typical sites include the liver, spleen, and lymph nodes; however, craniofacial bone involvement and nasopharyngeal soft tissue masses are infrequently reported [2]. Such atypical presentations may resemble adenoid hypertrophy, malignancy, or chronic infection, resulting in delayed or incorrect diagnosis.
This case report describes a unique pediatric presentation of extramedullary erythropoiesis involving the skull and adenoidal region in a 3-year-old child, emphasizing the diagnostic challenges, radiological findings, and multidisciplinary management required for optimal outcomes.
Case Report
Patient History
A 3-year-old male child was brought to the pediatric outpatient department with complaints of sudden-onset fever for three days, accompanied by nasal obstruction, mouth breathing, and noisy breathing during sleep. The fever was intermittent, low to moderate grade, and not associated with chills, rigors, rash, or seizures.
The caregivers reported persistent mouth breathing and snoring over the preceding two months, suggestive of adenoid enlargement. There was no history of recurrent upper respiratory tract infections, epistaxis, weight loss, night sweats, or contact with tuberculosis.
On further inquiry, the parents noted intermittent pallor and easy fatigability over the last six months. There was no prior hospital admission or known diagnosis of anemia. Family history was unremarkable for hematological disorders, and there was no consanguinity.
Clinical Examination
On examination, the child appeared pale and febrile, with a temperature of 38.2°C. Vital signs were stable. Anthropometric measurements were appropriate for age.
Otorhinolaryngological examination revealed features consistent with adenoid hypertrophy, including nasal speech and reduced nasal airflow. There was no cervical lymphadenopathy. Systemic examination showed mild hepatosplenomegaly on deep palpation, which was not previously noted by caregivers.
There were no focal neurological deficits, skeletal deformities, or signs of bleeding. Cardiovascular and respiratory examinations were otherwise unremarkable.
Clinical Evaluation
Initial Differential Diagnosis
Based on the presenting symptoms, the initial differential diagnoses included:
-
Adenoid hypertrophy with intercurrent infection
-
Chronic upper airway obstruction
-
Hematological malignancy
-
Storage disorder
-
Chronic hemolytic anemia with secondary changes
The presence of pallor and hepatosplenomegaly prompted further hematological evaluation.
Investigations
Laboratory Studies
Baseline laboratory investigations revealed the following:
-
Hemoglobin: 7.6 g/dL
-
Mean corpuscular volume: 62 fL
-
Mean corpuscular hemoglobin: Reduced
-
Reticulocyte count: Elevated (4.8%)
-
White blood cell count: Mildly elevated
-
Platelet count: Normal
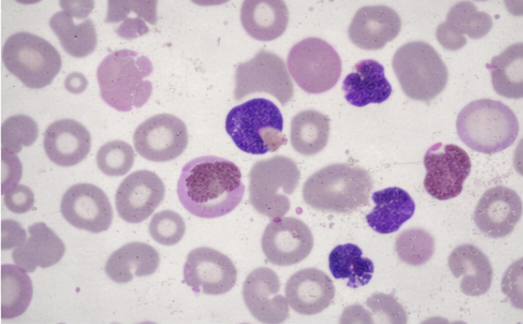
Peripheral blood smear demonstrated microcytic hypochromic anemia with anisopoikilocytosis, target cells, and occasional nucleated red blood cells, suggestive of a chronic hemolytic process.
C-reactive protein was mildly elevated, correlating with the febrile episode. Liver and renal function tests were within normal limits.
Radiological Evaluation
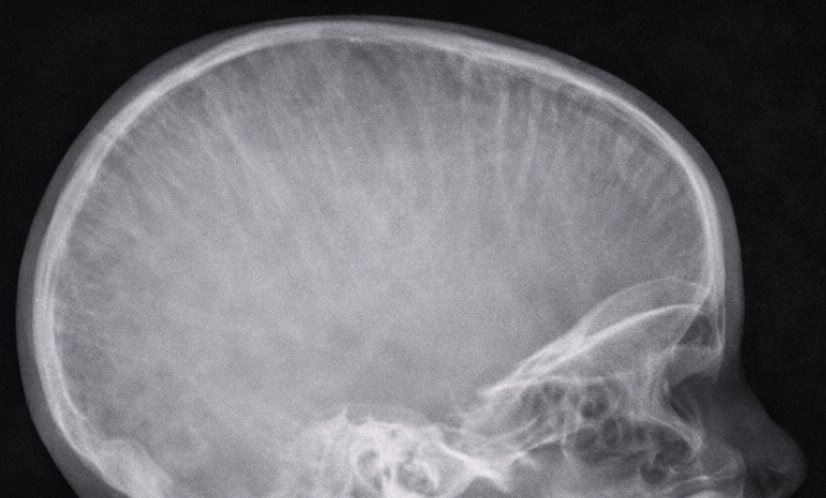
A lateral X-ray of the skull and nasopharynx was obtained to assess adenoid hypertrophy.

The radiograph demonstrated:
-
Prominent widening of the diploic spaces
-
Vertical striations giving a characteristic “hair-on-end” appearance
-
Soft tissue prominence in the nasopharyngeal region
These findings raised suspicion of marrow hyperplasia rather than isolated lymphoid hypertrophy.
Ultrasound of the abdomen revealed mild hepatosplenomegaly without focal lesions.

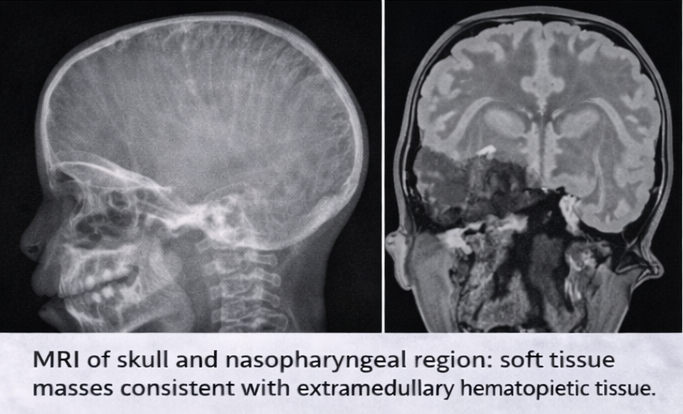
Magnetic resonance imaging (MRI) of the skull and nasopharynx showed soft tissue masses with signal characteristics consistent with extramedullary hematopoietic tissue involving the skull bones and nasopharyngeal region, without evidence of malignancy or abscess formation.
Diagnosis
Based on the clinical presentation, laboratory findings of chronic hemolytic anemia, and characteristic radiological features, a diagnosis of extramedullary erythropoiesis involving the skull and adenoidal region was established.
Further hematological evaluation, including hemoglobin electrophoresis, confirmed a diagnosis of β-thalassemia intermedia, explaining the chronic ineffective erythropoiesis and compensatory extramedullary hematopoietic activity.
Management and Outcome
Multidisciplinary Approach
The child was managed through a coordinated multidisciplinary approach involving pediatric hematology, otorhinolaryngology, radiology, and general pediatrics. Detailed counseling sessions were conducted with the caregivers to explain the nature of the condition, its chronic course, and the rationale for management decisions.
Therapeutic Management
The child received packed red blood cell transfusion to correct symptomatic anemia. Antipyretics were administered for fever, which resolved within 48 hours.
Given that the nasopharyngeal mass represented extramedullary erythropoiesis rather than isolated adenoid hypertrophy, surgical intervention was deferred to avoid unnecessary bleeding and complications. The child was initiated on folic acid supplementation and scheduled for regular hematological monitoring.
Follow-Up
Serial follow-up visits demonstrated clinical improvement, with reduction in nasal obstruction and improved activity levels. Hemoglobin levels stabilized following transfusion support. Repeat imaging at three months showed partial regression of extramedullary hematopoietic tissue.
The child continues under long-term hematology follow-up, with ongoing assessment for transfusion requirements and disease-modifying strategies.
Discussion
Extramedullary erythropoiesis is an adaptive response to chronic anemia and ineffective erythropoiesis. In pediatric patients, its occurrence often signals an underlying hematological disorder that may remain undiagnosed until complications arise [3].
Craniofacial involvement is rare and may present with airway obstruction, facial swelling, or radiological abnormalities. The “hair-on-end” appearance on skull radiographs is a classic but uncommon finding in modern clinical practice, reflecting marrow expansion secondary to increased erythropoietic demand [4].
This case emphasizes the importance of considering hematological causes in children presenting with adenoid hypertrophy and anemia. Early recognition prevents unnecessary surgical intervention and allows timely institution of appropriate hematological management.
Conclusion
Extramedullary erythropoiesis is a rare but important diagnostic consideration in anemic children presenting with atypical craniofacial or nasopharyngeal findings. A systematic approach incorporating clinical evaluation, laboratory assessment, and imaging is essential for accurate diagnosis. Multidisciplinary management and caregiver education play a crucial role in achieving favorable outcomes and preventing avoidable procedures.
References
-
Hoffbrand AV, Moss PAH. Essential Haematology. 7th ed. Wiley-Blackwell; 2016.
-
Taher AT, et al. Extramedullary hematopoiesis in thalassemia: clinical implications. Blood Rev. 2018;32(1):1–8.
-
Musallam KM, et al. Non-transfusion-dependent thalassemias. Haematologica. 2013;98(6):833–844.
-
Cappellini MD, Cohen A, Porter J, et al. Guidelines for the Management of Thalassemia. Thalassemia International Federation; 2021.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Examines Office-Based Transperineal Prostate Biopsies Methodology.
2.
A global study demonstrates that screening for lung cancer significantly raises the long-term survival rate.
3.
Is a $2,000 Whole-Body MRI Worth It?
4.
Surgery may not be necessary to treat invasive breast cancer
5.
Limited Benefit from New Drugs; Significant Increase in Drug Prices; AI Boost for Mammo Results.
1.
Understanding Evans Syndrome: Causes, Symptoms, and Treatment Options
2.
Understanding Sepsis and Precision-Medicine-Based Immunotherapy: A Pathophysiological Perspective
3.
Exploring The Science Of Hematopoietic Stem Cell Transplantation: What You Need To Know
4.
Unlocking the Secret to Accurate ANC Calculation with This Informative Blog Post
5.
Understanding Lymphedema: Symptoms, Causes, and Treatment
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Pazopanib: A Game-Changer in Managing Advanced Renal Cell Carcinoma - Part VI
2.
Rates of CR/CRi and MRD Negativity in Iontuzumab-Treated Patients
3.
Management of 1st line ALK+ mNSCLC (CROWN TRIAL Update) - Part II
4.
First-Line Maintenance Therapy for Metastatic Urothelial Carcinoma: Bridging Clinical Practice and Trials
5.
Recent Data Analysis for First-Line Treatment of ALK+ NSCLC: A Final Discussion

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge