Maculopathy: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Maculopathy encompasses a heterogeneous group of disorders affecting the macula, the central region of the retina responsible for detailed vision. These conditions may result from metabolic, degenerative, inflammatory, vascular, or drug-related causes and can lead to significant visual impairment if not diagnosed and managed promptly. Patients typically present with central visual disturbances, including blurring, metamorphopsia, or scotomas. Accurate diagnosis relies on detailed clinical examination supplemented by multimodal retinal imaging, particularly optical coherence tomography (OCT) and fundus fluorescein angiography (FFA). This case report describes an adult patient presenting with non-neovascular maculopathy, highlighting clinical features, diagnostic evaluation, management strategy, and visual outcomes, with emphasis on differential diagnosis and long-term monitoring.
Introduction
The macula is a specialized area of the retina responsible for central vision, color discrimination, and high-resolution visual acuity. Maculopathy refers to pathological conditions affecting this region and includes a wide spectrum of entities such as age-related macular degeneration (AMD), drug-induced maculopathy, diabetic macular disease, central serous chorioretinopathy, and inherited retinal disorders. Depending on etiology and severity, maculopathy can significantly impair daily activities such as reading, driving, and facial recognition.
The clinical relevance of maculopathy lies in its often insidious onset and potential for irreversible visual loss if diagnosis is delayed. Advances in retinal imaging have improved early detection and classification, enabling timely intervention and improved prognosis. This report presents a case of idiopathic non-neovascular maculopathy in a middle-aged patient, outlining the diagnostic process, management approach, and clinical outcome.
Case Report
Patient History
A 52-year-old male presented to the ophthalmology outpatient department with complaints of gradual, painless diminution of vision in his right eye over a period of six months. He described difficulty reading fine print and noted distortion of straight lines, particularly when using the affected eye alone. There was no history of sudden vision loss, flashes, floaters, ocular pain, redness, or trauma.
The patient had no known history of diabetes mellitus or hypertension. He was not on long-term systemic medications and denied exposure to drugs known to cause retinal toxicity, such as chloroquine or hydroxychloroquine. There was no history of steroid use. Family history was negative for hereditary retinal disorders. He was a non-smoker and reported no occupational exposure to retinal toxins.
Clinical Examination
On examination, best-corrected visual acuity (BCVA) was 6/12 in the right eye and 6/6 in the left eye. Anterior segment examination of both eyes was unremarkable, with clear cornea, normal anterior chamber depth, and reactive pupils. Intraocular pressure measured by applanation tonometry was within normal limits in both eyes.
Dilated fundus examination of the right eye revealed subtle loss of foveal reflex with mild retinal pigment epithelial (RPE) mottling in the macular region.
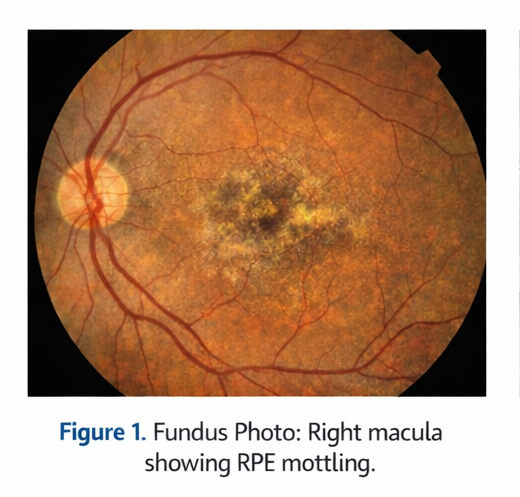
No hemorrhages, hard exudates, or drusen were noted. The peripheral retina was normal. Fundus examination of the left eye was within normal limits.
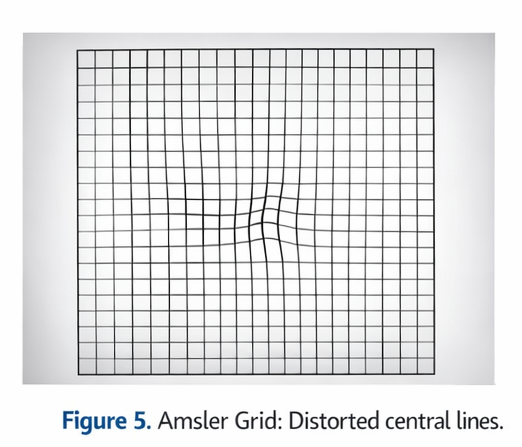
Amsler grid testing demonstrated mild metamorphopsia in the central field of the right eye, while the left eye showed no abnormalities.
Clinical Evaluation
Differential Diagnosis
Based on the clinical findings, the following differential diagnoses were considered:
- Non-neovascular (dry) maculopathy
- Early age-related macular degeneration
- Central serous chorioretinopathy (chronic variant)
- Drug-induced maculopathy
- Macular dystrophy
The absence of subretinal fluid on clinical examination and lack of systemic risk factors helped narrow the provisional diagnosis toward non-neovascular maculopathy.
Investigations
Optical Coherence Tomography (OCT)
Spectral-domain OCT of the right eye demonstrated focal disruption of the ellipsoid zone with mild thinning of the outer retinal layers at the fovea. There was no evidence of intraretinal or subretinal fluid. The retinal pigment epithelium appeared irregular but intact. OCT of the left eye was normal.

Fundus Fluorescein Angiography (FFA)
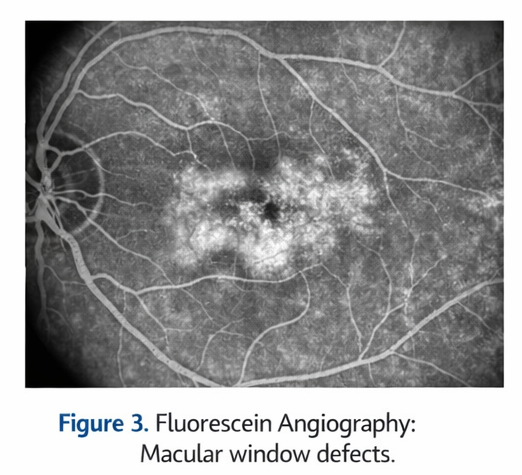
FFA showed mild window defects corresponding to areas of RPE alteration in the macula of the right eye without evidence of leakage, neovascularization, or pooling. These findings ruled out neovascular AMD and active central serous chorioretinopathy.
Fundus Autofluorescence (FAF)
FAF imaging demonstrated focal areas of hypoautofluorescence at the macula, consistent with localized RPE dysfunction.
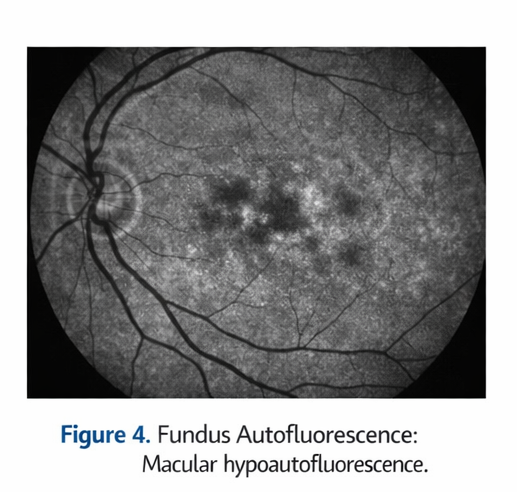
The imaging findings supported a diagnosis of non-neovascular maculopathy.
Management and Outcome
Treatment Planning
Given the non-neovascular nature of the maculopathy and absence of treatable exudative changes, conservative management with close monitoring was advised. The patient was counseled regarding the nature of the disease, prognosis, and importance of regular follow-up.
Medical Management
The patient was advised antioxidant supplementation containing lutein and zeaxanthin, along with omega-3 fatty acids, as supportive therapy. Lifestyle modifications, including protection from excessive sunlight and maintaining a balanced diet rich in leafy green vegetables, were recommended.
The patient was instructed on daily Amsler grid self-monitoring and advised to report any sudden worsening of vision or distortion.
Follow-Up and Outcome
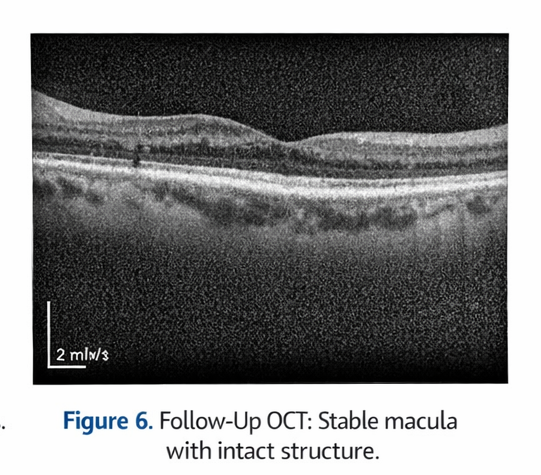
At three-month follow-up, the patient reported subjective stabilization of visual symptoms. BCVA remained 6/12 in the right eye. Repeat OCT showed no progression of outer retinal changes and no development of subretinal fluid.
At six-month follow-up, visual acuity remained stable, and fundus findings were unchanged. There was no evidence of progression to neovascular disease. The patient expressed satisfaction with the counseling and management approach.
Discussion
Maculopathy represents a diverse group of disorders with varying etiologies and prognoses. Non-neovascular maculopathy is often characterized by subtle RPE and photoreceptor changes that may cause gradual visual deterioration. OCT plays a pivotal role in identifying early structural changes and excluding treatable causes such as choroidal neovascularization.
Differentiating non-neovascular maculopathy from early AMD and central serous chorioretinopathy can be challenging, particularly in cases with overlapping features. Multimodal imaging, including OCT, FFA, and FAF, is essential for accurate diagnosis. Histopathological confirmation is rarely required in maculopathy, unlike osseous or soft tissue lesions.
Management primarily focuses on observation, risk factor modification, and patient education. While no definitive curative therapy exists for many non-neovascular maculopathies, early diagnosis and regular monitoring can help prevent progression and detect complications at a treatable stage.
The prognosis is generally favorable in stable, non-progressive cases, though long-term follow-up is recommended due to the potential for progression or development of neovascular changes.
Conclusion
Maculopathy is a clinically significant retinal condition that can result in central visual impairment. Accurate diagnosis requires careful clinical assessment and multimodal retinal imaging. Conservative management with close observation is appropriate in non-neovascular cases. Patient education and regular follow-up are essential to ensure early detection of progression and preservation of visual function.
References
- Spaide RF, Curcio CA. Anatomy of the choroid, retina, and macula. Prog Retin Eye Res. 2011. https://pubmed.ncbi.nlm.nih.gov/21600938/
- Ferris FL, Wilkinson CP, Bird A, et al. Clinical classification of age-related macular degeneration. Ophthalmology. 2013. https://pubmed.ncbi.nlm.nih.gov/23332590/
- Freund KB, Mrejen S, Gallego-Pinazo R. An update on central serous chorioretinopathy. Surv Ophthalmol. 2015. https://pubmed.ncbi.nlm.nih.gov/25135442/
- Holz FG, Schmitz-Valckenberg S, Fleckenstein M. Recent developments in the diagnosis and monitoring of macular disease. Ophthalmologica. 2014. https://pubmed.ncbi.nlm.nih.gov/24614464
- Schmitz-Valckenberg S, Holz FG, Bird AC, Spaide RF. Fundus autofluorescence imaging: review and perspectives. Retina. 2008 https://pubmed.ncbi.nlm.nih.gov/18536603/
- Chew EY, Clemons TE, Sangiovanni JP, et al. Secondary analyses of the AREDS2 randomized clinical trial. JAMA Ophthalmol. 2014. https://jamanetwork.com/journals/jamaophthalmology/fullarticle/1893665
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Nuclear missile workers are contracting cancer: They blame the bases
2.
Mixed Results With Cyclophosphamide in Mismatched Unrelated Stem Cell Transplants
3.
New analysis helps discern benign from malignant thyroid growths
4.
MCh in Gynecologic Oncology: Admission, Medical School, Fees, Qualifications Information
5.
Even a few mutated cells can significantly impact how blood cancers develop, study finds
1.
Uncovering the Hidden Signs: How to Recognize the Early Symptoms of Colon Cancer
2.
The benefits and risks of taking fludrocortisone for adrenal insufficiency
3.
IGSF8: A Rising Star in Cancer Immunotherapy - Harnessing the Innate Immune System
4.
Innovative Intraoperative Therapies in Neurosurgical Oncology: Advancing Precision and Outcomes
5.
Different Types of Blood Dyscrasias
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
An In-Depth Look At The Signs And Symptoms Of Lymphoma
2.
Iron Deficiency Anemia: Ferric Maltol As a New Treatment Option- Further Discussion on A New Perspective
3.
Revolutionizing Treatment of ALK Rearranged NSCLC with Lorlatinib - Part VII
4.
Virtual Case Study on Pedal Edema and Triple Vessel Disease - An Initiative by Hidoc Dr.
5.
Nimotozumab Plus Chemo-radiotherapy v/s Placebo Plus Chemo-radiotherapy in Locally Advanced Nasopharyngeal Carcinoma

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge