Acute Pulmonary Edema: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes - A Case Report
OthersPage Navigation
Abstract
Acute pulmonary edema (APE) is a life-threatening condition characterized by rapid accumulation of fluid in the alveolar spaces, leading to severe respiratory distress and hypoxemia. It may result from cardiogenic causes, most commonly acute decompensated heart failure, or non-cardiogenic etiologies such as acute respiratory distress syndrome, fluid overload, or high-altitude exposure. Clinical manifestations include sudden onset dyspnea, orthopnea, paroxysmal nocturnal dyspnea, cough with frothy sputum, and signs of sympathetic activation such as tachycardia and diaphoresis. Prompt recognition, stabilization, and targeted therapy are critical to reduce morbidity and mortality. We report a case of acute cardiogenic pulmonary edema in an elderly male presenting with sudden shortness of breath, hypoxemia, and pulmonary crackles. The case highlights clinical presentation, diagnostic evaluation including imaging and laboratory assessment, immediate management with oxygen, diuretics, and vasodilators, and short-term outcomes. Early intervention, etiologic treatment, and close monitoring remain essential to optimize patient recovery and prevent recurrence.
Introduction
Acute pulmonary edema is defined as rapid accumulation of extravascular fluid in the lungs, leading to impaired gas exchange and acute respiratory distress. Cardiogenic pulmonary edema, caused by elevated pulmonary capillary wedge pressure due to left ventricular dysfunction, accounts for the majority of cases. Non-cardiogenic pulmonary edema arises from increased alveolar-capillary permeability or fluid overload. Common risk factors include hypertension, ischemic heart disease, valvular heart disease, and chronic kidney disease. Clinical consequences range from mild dyspnea to severe hypoxemia, respiratory failure, and hemodynamic instability. Early recognition and prompt management, guided by clinical assessment, imaging, and laboratory data, are critical to reduce morbidity and mortality.
Case Report
Patient History
A 68-year-old male with a history of chronic hypertension and ischemic heart disease presented to the emergency department with sudden onset shortness of breath, orthopnea, and productive cough with pink frothy sputum for 3 hours. He reported associated palpitations and profuse sweating. There was no history of chest trauma or recent infection. The patient had not been adherent to his antihypertensive and heart failure medications in the preceding week. He denied fever or hemoptysis. Past medical history included a prior myocardial infarction 5 years ago and stable chronic kidney disease stage 2.
Clinical Examination
On examination, the patient was in severe respiratory distress, using accessory muscles of respiration. Vital signs: blood pressure 180/100 mmHg, heart rate 112 bpm, respiratory rate 32/min, oxygen saturation 84% on room air. Jugular venous distension was noted. Lung auscultation revealed bilateral basal and mid-lung crepitations with occasional wheezes.
Cardiac examination showed an S3 gallop. Peripheral edema was present in both lower limbs. Neurological and abdominal examinations were unremarkable.
Clinical Evaluation
Differential Diagnosis
- Cardiogenic pulmonary edema secondary to acute decompensated heart failure
- Acute exacerbation of chronic obstructive pulmonary disease with fluid overload
- Pneumonia with acute respiratory distress
- Acute respiratory distress syndrome (non-cardiogenic)
- Pulmonary embolism with right heart strain
Investigations
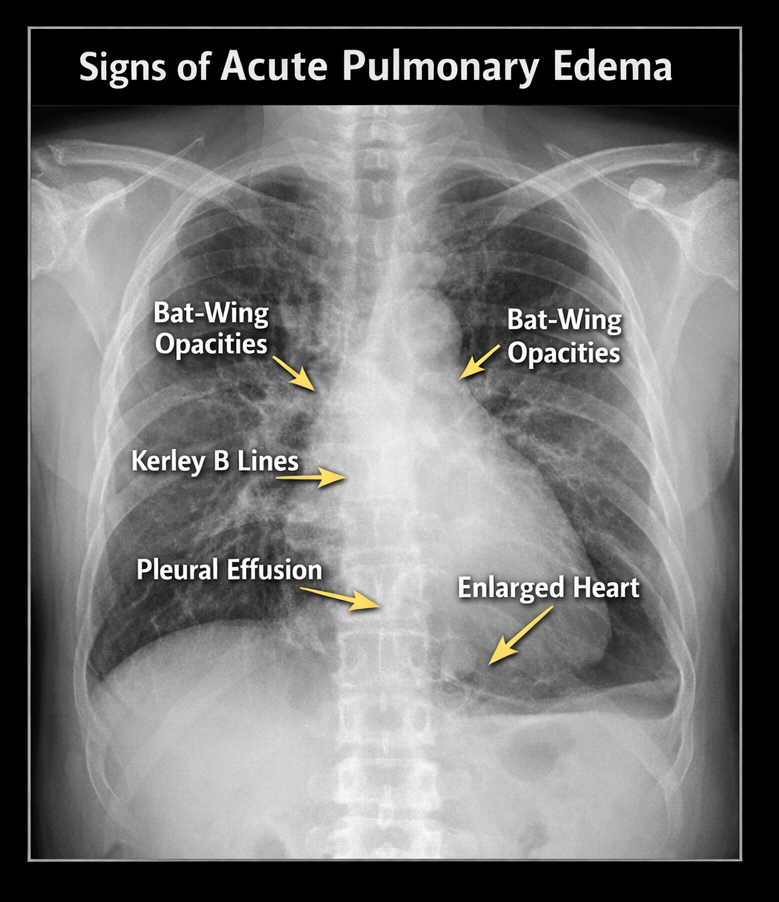
- Chest X-ray: Bilateral alveolar infiltrates, pulmonary venous congestion, and cardiomegaly
- Electrocardiogram (ECG): Sinus tachycardia, left ventricular hypertrophy, nonspecific ST-T changes
- Echocardiogram: Reduced left ventricular ejection fraction (35%), global hypokinesia
- Laboratory: Elevated BNP (1250 pg/mL), mild renal impairment (creatinine 1.5 mg/dL), normal troponin
- Arterial blood gas: Hypoxemia with PaO₂ 55 mmHg, respiratory alkalosis
Management and Outcome
Management Strategy
Immediate stabilization included:
- High-flow oxygen therapy via face mask to maintain SpO₂ > 92%
- Intravenous loop diuretic (furosemide 40 mg IV bolus, followed by infusion)

- Intravenous nitroglycerin infusion for blood pressure control and preload reduction
- Morphine 2 mg IV for anxiety and dyspnea relief
- Continuous cardiac and oxygen saturation monitoring in ICU
The patient was positioned upright to reduce venous return and improve ventilation. Strict fluid balance and daily weights were monitored. Once stabilized, oral heart failure medications (ACE inhibitor, beta-blocker) were optimized, and patient education on adherence was provided.
Follow-Up and Outcome
Within 24 hours, the patient showed marked symptomatic improvement, with reduced dyspnea and SpO₂ rising to 95% on supplemental oxygen. Repeat chest X-ray showed partial resolution of pulmonary congestion. By day 3, the patient was hemodynamically stable and transitioned to oral diuretics and home heart failure management. At 1-month follow-up, he reported improved exercise tolerance and adherence to heart failure medications, with no recurrence of acute pulmonary edema.
Discussion
Acute pulmonary edema is a life-threatening medical emergency that demands rapid recognition, prompt diagnostic evaluation, and immediate therapeutic intervention to prevent hypoxemia, respiratory failure, and hemodynamic collapse. A cardiogenic etiology should be strongly suspected in patients with a known history of ischemic heart disease, heart failure, valvular heart disease, cardiomyopathy, uncontrolled hypertension, or recent myocardial infarction, particularly when accompanied by acute severe dyspnea, orthopnea, frothy sputum, elevated blood pressure, raised jugular venous pressure, basal crackles, peripheral edema, and other clinical signs of volume overload. Bedside clinical assessment supported by continuous pulse oximetry and arterial blood gas analysis guides initial stabilization, while chest radiography typically demonstrates bilateral alveolar infiltrates and vascular congestion; echocardiography provides critical information on left ventricular systolic and diastolic function, valvular abnormalities, and filling pressures. Cardiac biomarkers and natriuretic peptides such as B-type natriuretic peptide (BNP) or NT-proBNP aid in differentiating cardiogenic from non-cardiogenic causes and in risk stratification, while electrocardiography and cardiac troponins help identify acute coronary syndromes as precipitating factors.
Management prioritizes rapid improvement in oxygenation and ventilation using supplemental oxygen, high-flow nasal oxygen, or non-invasive ventilation (CPAP/BiPAP) to reduce work of breathing and preload, with early endotracheal intubation reserved for refractory respiratory distress or altered mental status. Hemodynamic optimization includes preload reduction with intravenous loop diuretics, afterload reduction with vasodilators (e.g., nitrates) in hypertensive patients, and cautious use of inotropes in selected cases of low-output states with hypotension. Concomitant treatment of the underlying cardiac precipitant—such as acute coronary syndrome, hypertensive emergency, arrhythmias, acute valvular dysfunction, or fluid overload—is essential for definitive control. Non-pharmacologic measures, including upright positioning to improve ventilation-perfusion matching, fluid and sodium restriction, careful monitoring of urine output, and early mobilization once stabilized, contribute to symptomatic relief and prevention of recurrence. Early, protocol-driven intervention reduces morbidity and mortality, shortens intensive care stay, prevents progression to respiratory failure and multiorgan dysfunction, and improves both short- and long-term outcomes. Multidisciplinary care involving cardiology, critical care, emergency medicine, nursing, respiratory therapy, and structured patient education on medication adherence, dietary modification, blood pressure control, and early symptom recognition is crucial to reduce readmissions, prevent recurrent decompensation, and optimize long-term quality of life.
Conclusion
Acute pulmonary edema is a life-threatening complication of cardiac dysfunction that requires prompt recognition and aggressive management. It results from elevated left ventricular pressures causing fluid accumulation in the alveoli, leading to severe hypoxemia and respiratory distress. Early stabilization with oxygen therapy, diuretics, vasodilators, and supportive measures, such as upright positioning, can rapidly improve respiratory and hemodynamic status. Identification and treatment of underlying causes, including myocardial ischemia, arrhythmias, or valvular disease, are essential to prevent recurrence.
Long-term management focuses on optimization of heart failure therapy, lifestyle modifications, and patient education on medication adherence, symptom monitoring, and early warning signs. Multidisciplinary follow-up involving cardiology, nursing, and physiotherapy improves functional outcomes, reduces hospital readmissions, and enhances quality of life. Comprehensive care stabilizes acute episodes and supports sustained improvements in morbidity, prognosis, and overall patient well-being.
References
- Gheorghiade M, Pang PS. Acute heart failure syndromes. J Am Coll Cardiol. 2009;53(7):557–573.
- Ponikowski P, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2022;43(36):3599–3726.
- Bhattacharya M, et al. Acute pulmonary edema: Clinical features, management, and outcomes. Indian Heart J. 2020;72(4):343–352.
- Cotter G, et al. Management of acute pulmonary edema. Circulation. 2008;117:1977–1990.
- Masip J, et al. Noninvasive ventilation in acute cardiogenic pulmonary edema. N Engl J Med. 2000;342:145–149.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Sub-Q Ketamine is Safe and Very Effective for Severe Depression.
2.
Study indicates that exercise can help colon cancer survivors live as long as matched individuals
3.
Contradictory Results Are Found in Two Pembrolizumab Trials for Head and Neck Cancer.
4.
Can Concurrent Boost Safely Shorten Breast Cancer Radiation?
5.
Positive Trials; Malignancies Increasing in Younger Adults; Andre Braugher's Cancer Dx.
1.
Trends in Incidence, Care, and Surgery for Medullary Thyroid Cancer: A Review
2.
Antibody-Drug Conjugates in Oncology: Breakthroughs, Clinical Updates, and Pipeline Innovation
3.
Navigating the Stages of Thyroid Cancer: A Guide for Patients
4.
Polycythemia Vera: A Historical Perspective and Contemporary Management
5.
Glofitamab: A Breakthrough Therapy for Relapsed/Refractory Mantle Cell Lymphoma
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Pazopanib: A Game-Changer in Managing Advanced Renal Cell Carcinoma - Part IV
2.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VIII
3.
Evolving Space of First-Line Treatment for Urothelial Carcinoma- Case Discussion
4.
Key Takeaways from The CROWN Trial For ALK + NSCLC Patients with CNS Diseases
5.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part I

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge