Preeclampsia: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Preeclampsia is a pregnancy-specific hypertensive disorder characterized by new-onset hypertension and signs of maternal organ dysfunction after 20 weeks of gestation. It remains a major cause of maternal and perinatal morbidity and mortality worldwide. Patients commonly present with elevated blood pressure, proteinuria, headache, visual disturbances, and edema. Diagnosis is based on clinical assessment, blood pressure measurements, and laboratory evaluation for proteinuria and organ involvement. Early recognition and timely management are critical to prevent complications such as eclampsia, placental abruption, and fetal growth restriction. This report describes a case of preeclampsia in a third-trimester pregnant woman that was successfully managed with antihypertensive therapy, close monitoring, and timely delivery.
Introduction
Preeclampsia is a multisystem disorder unique to pregnancy, typically developing after 20 weeks of gestation in previously normotensive women. It is characterized by hypertension and evidence of end-organ dysfunction, most commonly proteinuria.
The exact pathophysiology remains incompletely understood but is believed to involve abnormal placental implantation, endothelial dysfunction, and systemic inflammatory responses. These changes lead to widespread vasoconstriction, increased vascular permeability, and reduced organ perfusion.
Risk factors include first pregnancy, advanced maternal age, obesity, chronic hypertension, diabetes mellitus, and multiple gestations. Clinical manifestations may range from mild hypertension to severe disease with complications such as eclampsia, HELLP syndrome, and fetal growth restriction.
Early diagnosis and careful monitoring are essential to ensure maternal safety and optimize fetal outcomes. This report presents a case of preeclampsia diagnosed during the third trimester and managed successfully with appropriate medical care.
Case Report
Patient History
A 28-year-old primigravida at 32 weeks of gestation presented to the obstetrics clinic with complaints of persistent headache and swelling of the face and feet for the past five days.
The patient also reported occasional blurred vision and fatigue. There was no history of seizures, abdominal trauma, or vaginal bleeding. Her antenatal course had been uncomplicated until the current visit.
She had no prior history of chronic hypertension, renal disease, or diabetes mellitus.
Clinical Examination
On examination, the patient was alert and afebrile.
Vital signs revealed:
- Blood pressure: 158/98 mmHg
- Pulse rate: 88 beats per minute
- Respiratory rate: 18 breaths per minute
Physical examination showed bilateral pedal edema and mild facial puffiness.
Obstetric examination revealed a uterine size consistent with gestational age and a fetal heart rate of 142 beats per minute. No uterine tenderness was noted.
Clinical Evaluation
Differential Diagnosis
Based on clinical findings, the following conditions were considered:
• Gestational hypertension
• Preeclampsia
• Chronic hypertension in pregnancy
• Renal disease associated with pregnancy
Further investigations were performed to establish the diagnosis.
Investigations
Blood Pressure Monitoring
Repeated measurements confirmed persistent hypertension ≥140/90 mmHg.

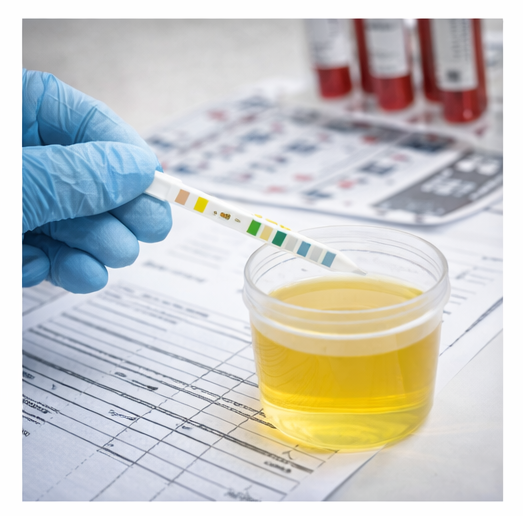
Urinalysis
Dipstick testing revealed proteinuria (+2).
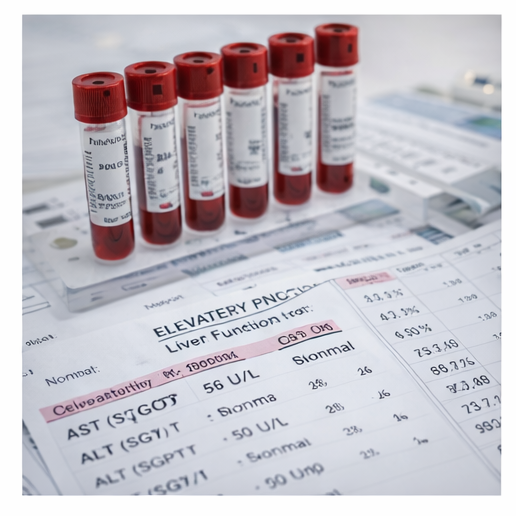
Laboratory Tests
- Hemoglobin: within normal limits
- Platelet count: normal
- Liver function tests: mildly elevated transaminases
- Serum creatinine: within normal limits
Obstetric Ultrasound
Ultrasound examination showed a single live intrauterine fetus with appropriate growth for gestational age and normal amniotic fluid volume.
Diagnosis
Based on new-onset hypertension after 20 weeks of gestation accompanied by proteinuria, a diagnosis of preeclampsia was established.
Management and Outcome
Initial Management
The patient was admitted for close maternal and fetal monitoring. Management included:
• Antihypertensive therapy to control blood pressure

• Magnesium sulfate prophylaxis to prevent seizures
• Regular blood pressure monitoring
• Fetal monitoring with non-stress tests and ultrasound
• Advice regarding rest and dietary measures
Follow-Up and Outcome
Over the following week, the patient’s blood pressure gradually stabilized with appropriate antihypertensive therapy and close inpatient monitoring. Serial blood pressure recordings showed progressive improvement, and the patient reported relief from headache and visual disturbances. Regular fetal surveillance with non-stress testing and ultrasonography demonstrated reassuring fetal well-being, with stable fetal heart rate patterns and normal amniotic fluid volume.
At 37 weeks of gestation, labor was induced due to persistent hypertension and to minimize the risk of maternal and fetal complications. The patient underwent a closely monitored labor process and subsequently delivered a healthy newborn with good Apgar scores at 1 and 5 minutes. The neonate showed normal vital parameters and did not require any special care.
During the postpartum period, the patient continued to be monitored for blood pressure and potential complications related to hypertensive disorders of pregnancy. Her blood pressure gradually returned toward normal levels over the next few days with continued medical therapy and supportive care. Both the mother and the newborn remained clinically stable, and they were discharged in good condition with advice for postpartum follow-up and blood pressure monitoring.
Discussion
Preeclampsia is one of the most significant hypertensive disorders of pregnancy and contributes substantially to maternal and neonatal morbidity worldwide.
The condition is believed to result from abnormal placental development leading to endothelial dysfunction and systemic vasoconstriction. These pathophysiological changes result in hypertension and multiorgan involvement affecting the kidneys, liver, brain, and placenta.
Clinically, patients often present with hypertension, edema, headache, visual disturbances, and proteinuria. Severe disease may progress to eclampsia, HELLP syndrome, or placental abruption, which can threaten both maternal and fetal health.
Diagnosis is based primarily on blood pressure measurement and detection of proteinuria or other signs of organ dysfunction. Ultrasound and fetal monitoring are important to evaluate fetal well-being and detect complications such as growth restriction.
Management depends on disease severity and gestational age. Mild cases may be managed with close monitoring and antihypertensive therapy, whereas severe cases may require early delivery. Magnesium sulfate is widely used for seizure prophylaxis in patients with severe preeclampsia.
Timely recognition and appropriate management significantly improve outcomes for both mother and fetus.
Conclusion
Preeclampsia is a serious hypertensive disorder of pregnancy characterized by new-onset hypertension and organ involvement after 20 weeks of gestation. Early identification through routine antenatal monitoring is essential to prevent severe maternal and fetal complications.
Accurate diagnosis, careful blood pressure control, and close fetal surveillance are key components of management. Timely delivery remains the definitive treatment when maternal or fetal risks increase.
With prompt diagnosis, appropriate medical management, and regular follow-up, most patients with preeclampsia can achieve favorable maternal and neonatal outcomes.
References
- American College of Obstetricians and Gynecologists. Gestational hypertension and preeclampsia. Obstetrics & Gynecology. 2020. https://pubmed.ncbi.nlm.nih.gov/32804849/
- Roberts JM, Hubel CA. The two-stage model of preeclampsia. Placenta. 2009. https://pubmed.ncbi.nlm.nih.gov/19070896/
- Magee LA, et al. Diagnosis, evaluation, and management of hypertensive disorders of pregnancy. Pregnancy Hypertension. 2014. https://pubmed.ncbi.nlm.nih.gov/26104417/
- Phipps E, et al. Preeclampsia: pathogenesis, novel diagnostics, and therapies. Nature Reviews Nephrology. 2019. https://pubmed.ncbi.nlm.nih.gov/30683859/
- Brown MA, et al. Hypertensive disorders of pregnancy: ISSHP classification and management recommendations. Hypertension. 2018. https://pubmed.ncbi.nlm.nih.gov/29899139/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Sub-Q Ketamine is Safe and Very Effective for Severe Depression.
2.
Study indicates that exercise can help colon cancer survivors live as long as matched individuals
3.
Contradictory Results Are Found in Two Pembrolizumab Trials for Head and Neck Cancer.
4.
Can Concurrent Boost Safely Shorten Breast Cancer Radiation?
5.
Positive Trials; Malignancies Increasing in Younger Adults; Andre Braugher's Cancer Dx.
1.
Trends in Incidence, Care, and Surgery for Medullary Thyroid Cancer: A Review
2.
Antibody-Drug Conjugates in Oncology: Breakthroughs, Clinical Updates, and Pipeline Innovation
3.
Navigating the Stages of Thyroid Cancer: A Guide for Patients
4.
Polycythemia Vera: A Historical Perspective and Contemporary Management
5.
Glofitamab: A Breakthrough Therapy for Relapsed/Refractory Mantle Cell Lymphoma
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Pazopanib: A Game-Changer in Managing Advanced Renal Cell Carcinoma - Part IV
2.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VIII
3.
Evolving Space of First-Line Treatment for Urothelial Carcinoma- Case Discussion
4.
Key Takeaways from The CROWN Trial For ALK + NSCLC Patients with CNS Diseases
5.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part I

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge