Psoriasis: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes - A Case Report
OthersPage Navigation
Abstract
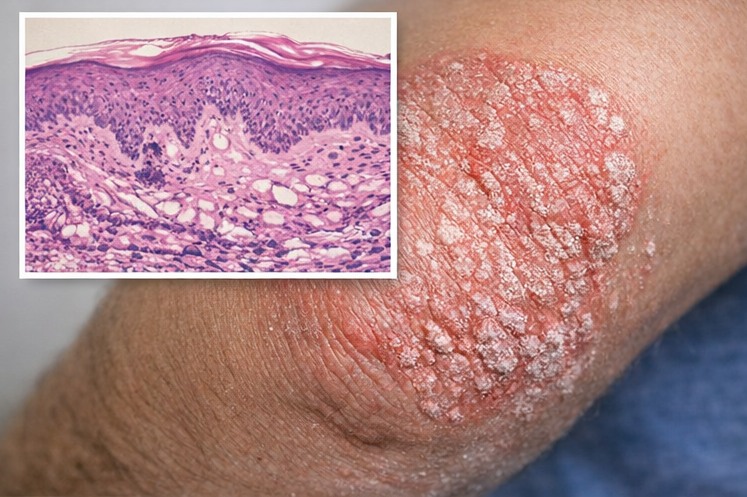
Psoriasis is a chronic, immune-mediated inflammatory skin disorder characterized by well-demarcated erythematous plaques with silvery scales. It affects approximately 2–3% of the global population and can present at any age, with significant physical, psychological, and social impact. The disease results from a complex interplay of genetic predisposition, immune dysregulation, and environmental triggers. Clinical manifestations range from localized plaque disease to extensive skin involvement with systemic complications such as psoriatic arthritis. Diagnosis is primarily clinical, supported by histopathology in atypical cases. Management is individualized based on disease severity, distribution, comorbidities, and patient preference, and includes topical therapy, phototherapy, systemic agents, and biologic therapies. This case report describes a pediatric patient with chronic plaque psoriasis, highlighting clinical features, diagnostic evaluation, management strategy, and short-term outcomes. Early diagnosis and appropriate treatment are essential to improve quality of life and prevent disease progression and complications.
Introduction
Psoriasis is a chronic, relapsing inflammatory dermatosis driven by T-cell–mediated immune mechanisms and abnormal keratinocyte proliferation. It commonly presents as chronic plaque psoriasis, although other variants such as guttate, pustular, erythrodermic, and inverse psoriasis are recognized. Pediatric psoriasis accounts for nearly one-third of cases, often posing diagnostic and therapeutic challenges.
Genetic susceptibility, particularly involving HLA-Cw6, combined with triggers such as infections, stress, trauma (Koebner phenomenon), and medications, contributes to disease onset and exacerbation. Psoriasis is increasingly recognized as a systemic inflammatory disorder associated with metabolic syndrome, cardiovascular disease, and psychosocial morbidity. This case report illustrates the clinical course and management of psoriasis in an adolescent patient, emphasizing early recognition and multidisciplinary care.
Case Report
Patient History
A 13-year-old male presented to the dermatology outpatient clinic with complaints of recurrent, itchy skin lesions over the scalp, elbows, and knees for the past six months. The lesions were gradually progressive and associated with mild pruritus but no pain or discharge. The patient reported worsening of symptoms during winter months.
There was no history of fever, recent infections, joint pain, or weight loss. Family history revealed that the patient’s father had a history of chronic plaque psoriasis. There was no history of drug intake, allergies, or systemic illness.
Clinical Examination
General physical examination was unremarkable, and vital signs were stable. Cutaneous examination revealed multiple well-defined erythematous plaques with overlying silvery-white scales over the scalp, extensor surfaces of the elbows, and knees.



Auspitz sign was positive. Nail examination showed mild pitting without onycholysis. No mucosal involvement was noted.
Musculoskeletal examination revealed no joint tenderness, swelling, or restriction of movement. Other systemic examinations were within normal limits.
Clinical Evaluation
Differential Diagnosis
The differential diagnosis for chronic scaly plaques in an adolescent included:
• Psoriasis
• Seborrheic dermatitis
• Atopic dermatitis
• Tinea corporis
• Pityriasis rosea
Investigations
• Laboratory tests: Complete blood count, liver and renal function tests were within normal limits
• Skin biopsy: Performed to confirm diagnosis, revealing acanthosis, elongated rete ridges, parakeratosis, Munro microabscesses, and dilated dermal capillaries, consistent with psoriasis
• Severity assessment: Psoriasis Area and Severity Index (PASI) score was calculated as 6.2, indicating mild-to-moderate disease
Management and Outcome
Management Strategy
Given the limited body surface area involvement and absence of systemic disease, a conservative treatment approach was adopted:
• Topical therapy: Combination of topical corticosteroids and vitamin D analogs applied to affected areas

• Scalp treatment: Medicated coal tar and salicylic acid shampoo
• Emollients: Regular use to maintain skin hydration
• Lifestyle counseling: Education regarding disease chronicity, trigger avoidance, and adherence to treatment
• Psychological support: Counseling provided to address self-esteem and social concerns
Follow-Up and Outcome
At six-week follow-up, the patient showed significant improvement in plaque thickness and scaling, with marked reduction in pruritus. PASI score reduced to 2.1. At three months, lesions were minimally active, and scalp involvement had resolved. No adverse effects were reported.
The patient was advised regular follow-up to monitor disease activity and early detection of psoriatic arthritis or relapse.
Discussion
Psoriasis in pediatric patients presents unique diagnostic and therapeutic challenges due to varied clinical morphology and long-term treatment considerations. Genetic predisposition plays a significant role, as highlighted by the positive family history in this case. Immune dysregulation involving Th1 and Th17 pathways leads to keratinocyte hyperproliferation and chronic inflammation.
Diagnosis is primarily clinical, with histopathology reserved for atypical presentations. Mild-to-moderate psoriasis can be effectively managed with topical agents, while systemic therapy and biologics are reserved for severe or refractory disease. Early intervention not only improves skin outcomes but also mitigates psychological distress and long-term comorbidities.
Patient education and family involvement are critical in pediatric psoriasis, ensuring adherence and realistic expectations regarding disease course.
Conclusion
Psoriasis is a chronic inflammatory skin disorder with significant physical and psychosocial impact, particularly in pediatric populations, where visible lesions can adversely affect self-esteem, social interactions, and overall emotional well-being. The disease often follows a relapsing–remitting course, requiring long-term management and regular follow-up. Early diagnosis is crucial, as prompt recognition allows timely initiation of therapy, minimizes disease burden, and reduces the risk of complications such as extensive skin involvement or progression to psoriatic arthritis.
Accurate assessment of disease severity, using standardized tools and clinical judgment, enables clinicians to tailor treatment strategies to individual patient needs. Individualized management should take into account the extent of skin involvement, symptom severity, patient age, comorbid conditions, treatment tolerability, and family preferences. In mild-to-moderate psoriasis, topical therapy remains the cornerstone of treatment and is often effective in achieving disease control when used consistently and appropriately. Adjunctive measures, including emollient use, trigger avoidance, and patient education, further enhance treatment outcomes.
Ongoing monitoring is essential to detect disease progression, treatment-related adverse effects, and potential systemic involvement. Regular follow-up also provides opportunities to address psychosocial concerns, reinforce adherence, and modify therapy as needed. A holistic, patient-centered approach—integrating medical management, psychological support, and lifestyle counseling—can significantly improve quality of life, promote long-term disease control, and help pediatric patients and their families cope effectively with the chronic nature of psoriasis.
References
- Griffiths, C. E. M., & Barker, J. N. W. N. (2007). Pathogenesis and clinical features of psoriasis. The Lancet, 370(9583), 263–271. https://doi.org/10.1016/S0140-6736(07)61128-3
- Lowes, M. A., Bowcock, A. M., & Krueger, J. G. (2007). Pathogenesis and therapy of psoriasis. Nature, 445(7130), 866–873.https://www.nature.com/articles/nature05663
- Nestle, F. O., Kaplan, D. H., & Barker, J. (2009). Psoriasis. New England Journal of Medicine, 361(5), 496–509. https://www.nejm.org/doi/full/10.1056/NEJMra0804595
- Kim, W. B., Jerome, D., & Yeung, J. (2017). Diagnosis and management of psoriasis. Canadian Family Physician, 63(4), 278–285. https://www.cfp.ca/content/63/4/278
- Bronckers, I. M. G. J., et al. (2015). Psoriasis in children and adolescents: Diagnosis, management, and comorbidities. Pediatric Drugs, 17(5), 373– 84 https://link.springer.com/article/10.1007/s40272-015-0140-5
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Breast density changes over time are associated with an increased risk of cancer.
2.
How the metastasis of cancer is driven by cellular plasticity.
3.
Belzutifan Combo Could be Second-Line Option in Advanced RCC
4.
Radioligand Shows Promise in Metastatic Hormone-Sensitive Prostate Cancer
5.
Research indicates that extended PSMA therapy is safe and effective for patients with prostate cancer.
1.
Essential Oncology Updates: Diagnosis, Treatment Advances, Tools & Education Resources
2.
Unlocking the Secrets of Hemoglobin: How It Works to Keep Us Healthy
3.
Uncovering the Mystery of the Sessile Serrated Adenoma
4.
Biomimetic Nanovesicles Target Senescent-Escape Cancer Stem Cells in Breast Cancer
5.
The Science Behind Thrombolytic Drugs and Their Benefits
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
From Relapse to Remission: Mapping the Treatment Journey in Adult R/R-Cell ALL - Part 2
2.
An Eagles View - Evidence-based Discussion on Iron Deficiency Anemia- Panel Discussion
3.
Molecular Contrast: EGFR Axon 19 vs. Exon 21 Mutations - Part VI
4.
The Reign of the CROWN Trial and the Dawn of a New Era in Frontline Management
5.
Dacomitinib Case Presentation: Baseline Treatment and Current Status

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge