Bowen’s Disease Presenting as a Gradually Enlarging Erythematous Scaly Plaque: A Case Report
OthersPage Navigation
Abstract
Bowen’s disease is a rare form of intraepidermal squamous cell carcinoma characterized by a persistent, slowly enlarging erythematous scaly plaque. Although progression is typically indolent, delayed diagnosis may lead to invasive squamous cell carcinoma. We report the case of a 58-year-old woman who presented with a gradually increasing, well-demarcated red scaly plaque over the lower limb. Clinical examination and histopathological evaluation confirmed the diagnosis of Bowen’s disease. The patient was managed successfully with local treatment, resulting in complete lesion resolution. This case highlights the importance of early recognition of chronic, non-healing scaly plaques and timely biopsy to prevent malignant progression.
Introduction
Bowen’s disease is an in situ form of squamous cell carcinoma confined to the epidermis, first described by John T. Bowen in 1912 [1]. It is characterized by a persistent erythematous, scaly, well-demarcated plaque that enlarges slowly over time. Although the condition remains intraepidermal, approximately 3–5% of cases may progress to invasive squamous cell carcinoma if left untreated [2].
The disease predominantly affects older adults and commonly occurs on sun-exposed areas such as the lower limbs, head, neck, and upper extremities, though it may also occur on covered sites [3]. Risk factors include chronic ultraviolet exposure, immunosuppression, arsenic exposure, human papillomavirus infection, and advancing age [4]. Because Bowen’s disease often mimics benign inflammatory dermatoses such as psoriasis or eczema, diagnosis is frequently delayed.
Early recognition and appropriate management are crucial to prevent invasion and achieve optimal outcomes. This case report describes a typical presentation of Bowen’s disease and discusses key diagnostic and therapeutic considerations relevant to routine dermatological practice.
Case Report
Patient History
A 58-year-old woman presented to the dermatology outpatient clinic with a history of a slowly enlarging skin lesion on her left lower leg for approximately eight months. The lesion began as a small, asymptomatic red patch and gradually increased in size. She reported mild occasional itching but denied pain, bleeding, ulceration, or discharge.

There was no history of trauma at the site. The patient had applied topical emollients and over-the-counter antifungal creams without improvement. She denied prior similar lesions. Her medical history was unremarkable, with no known immunosuppression or prior skin cancers. There was no occupational exposure to arsenic, and no personal or family history of malignancy.
Clinical Findings
Cutaneous examination revealed a single, well-defined erythematous plaque measuring approximately 3 × 2.5 cm over the anterior aspect of the left lower leg.

The surface was scaly and slightly crusted, with irregular but sharply demarcated margins. The lesion was non-tender, firm, and non-indurated. No ulceration or nodularity was noted.
The surrounding skin appeared normal. No regional lymphadenopathy was detected. Based on the chronicity and appearance of the lesion, a provisional diagnosis of Bowen’s disease was considered, with differentials including psoriasis, chronic eczema, superficial basal cell carcinoma, and tinea corporis.
Investigations
A punch biopsy was performed from the lesion margin.

Histopathological examination revealed full-thickness epidermal dysplasia with disordered keratinocyte maturation, nuclear pleomorphism, hyperchromasia, and increased mitotic activity.
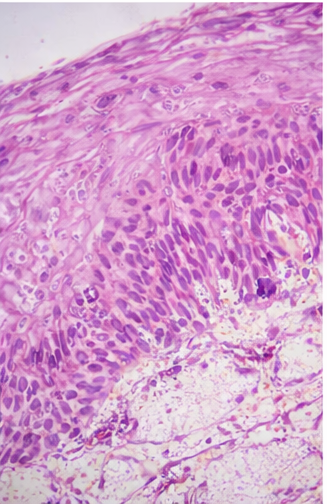
The basement membrane remained intact, with no evidence of dermal invasion. These findings were consistent with squamous cell carcinoma in situ (Bowen’s disease).
Routine laboratory investigations were within normal limits. No additional imaging was required, as there was no clinical suspicion of invasive disease.
Management and Outcome
The patient was counseled in detail regarding the diagnosis, natural history, prognosis, and available treatment options, including their potential benefits and adverse effects. Considering the localized nature, limited size of the lesion, and absence of clinical or histological evidence of invasion, a non-surgical approach was deemed appropriate. After shared decision-making, topical therapy was selected as the preferred treatment modality. The patient was initiated on topical 5-fluorouracil cream, applied once daily to the affected area for a duration of six weeks, with clear instructions regarding application technique and expected local reactions.

During treatment, the lesion demonstrated gradual and progressive regression, with reduction in erythema, scaling, and plaque thickness. Complete clinical resolution was observed by eight weeks. The patient experienced mild local erythema and scaling, which were anticipated adverse effects of topical chemotherapy and were managed conservatively with emollients and reassurance, without the need for treatment interruption. At follow-up visits conducted at three and six months, there was no clinical evidence of recurrence or progression.

The patient was counseled extensively on photoprotection strategies, including regular use of broad-spectrum sunscreen and avoidance of excessive sun exposure, and was enrolled in a schedule of regular dermatologic surveillance to facilitate early detection of any recurrence or new lesions.
Discussion
Bowen’s disease represents an early, non-invasive stage of squamous cell carcinoma, confined to the epidermis [2]. Clinically, it presents as a persistent, slowly enlarging erythematous scaly plaque, often mistaken for benign inflammatory conditions, leading to delayed diagnosis [3].
Histopathological confirmation remains the gold standard for diagnosis, as clinical features alone are not specific [4]. The hallmark feature is full-thickness epidermal atypia without invasion of the dermis. Early diagnosis is critical, as progression to invasive squamous cell carcinoma carries a risk of metastasis and increased morbidity.
Multiple treatment options are available, including surgical excision, topical chemotherapy (5-fluorouracil, imiquimod), cryotherapy, photodynamic therapy, and curettage with cautery [5]. Treatment selection depends on lesion size, location, patient comorbidities, and cosmetic considerations. When appropriately treated, prognosis is excellent.
Primary care physicians and dermatologists should maintain a high index of suspicion for Bowen’s disease when evaluating chronic, non-healing scaly plaques, particularly in older patients or sun-exposed areas.
Conclusion
Bowen’s disease is a rare but clinically significant precursor of invasive squamous cell carcinoma, representing an early intraepidermal stage in the malignant transformation of keratinocytes. Although the condition is generally slow growing, failure to recognize and treat it in a timely manner may allow progression to invasive disease, which carries a higher risk of local tissue destruction and potential metastasis. This case demonstrates a classic clinical presentation in the form of a gradually enlarging, well-demarcated erythematous scaly plaque, a morphology that is frequently misdiagnosed as a benign inflammatory dermatosis, leading to delayed intervention.
The report highlights the critical importance of maintaining a high index of suspicion and performing early biopsy for persistent or non-responsive cutaneous lesions, particularly in older individuals or lesions located on sun-exposed areas. Prompt histopathological confirmation enables appropriate therapeutic intervention at an early stage, resulting in excellent clinical outcomes and effective prevention of malignant progression. Increased awareness among primary care physicians and dermatologists is essential to minimize diagnostic delays, ensure timely management, and ultimately improve long-term patient prognosis through early detection and surveillance.
References
- Bowen JT. Precancerous dermatoses: a study of two cases of chronic atypical epithelial proliferation. J Cutan Dis. 1912;30:241–255.
- Cox NH, Eedy DJ, Morton CA. Guidelines for management of Bowen’s disease. Br J Dermatol. 1999;141(4):633–641.
- Nehal KS, Levine VJ. Cutaneous squamous cell carcinoma in situ (Bowen’s disease). J Am Acad Dermatol. 2001;45(5):684–696.
- Patel GK, Goodwin R, Chawla M, et al. Imiquimod 5% cream monotherapy for cutaneous squamous cell carcinoma in situ. Br J Dermatol. 2006;155(5):1025–1029.
- Morton CA, Birnie AJ, Eedy DJ. British Association of Dermatologists’ guidelines for the management of squamous cell carcinoma in situ (Bowen’s disease). Br J Dermatol. 2014;170(2):245–260.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Sub-Q Ketamine is Safe and Very Effective for Severe Depression.
2.
Study indicates that exercise can help colon cancer survivors live as long as matched individuals
3.
Contradictory Results Are Found in Two Pembrolizumab Trials for Head and Neck Cancer.
4.
Can Concurrent Boost Safely Shorten Breast Cancer Radiation?
5.
Positive Trials; Malignancies Increasing in Younger Adults; Andre Braugher's Cancer Dx.
1.
Trends in Incidence, Care, and Surgery for Medullary Thyroid Cancer: A Review
2.
Antibody-Drug Conjugates in Oncology: Breakthroughs, Clinical Updates, and Pipeline Innovation
3.
Navigating the Stages of Thyroid Cancer: A Guide for Patients
4.
Polycythemia Vera: A Historical Perspective and Contemporary Management
5.
Glofitamab: A Breakthrough Therapy for Relapsed/Refractory Mantle Cell Lymphoma
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Pazopanib: A Game-Changer in Managing Advanced Renal Cell Carcinoma - Part IV
2.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VIII
3.
Evolving Space of First-Line Treatment for Urothelial Carcinoma- Case Discussion
4.
Key Takeaways from The CROWN Trial For ALK + NSCLC Patients with CNS Diseases
5.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part I

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge