Ebola Virus Disease: Clinical Presentation, Diagnostic Challenges, Management, and Outcomes - A Case Report
OthersPage Navigation
Abstract
Ebola virus disease (EVD) is a severe, often fatal viral hemorrhagic fever caused by viruses of the genus Ebolavirus. It is characterized by acute onset of systemic illness with fever, gastrointestinal symptoms, coagulopathy, and multiorgan dysfunction. Although outbreaks are geographically concentrated in sub-Saharan Africa, globalization and international travel have increased the relevance of EVD to clinicians worldwide. Early diagnosis is challenging due to its nonspecific initial presentation, which overlaps with other tropical and febrile illnesses.
We report a confirmed case of Ebola virus disease in a young adult male presenting with acute febrile illness, gastrointestinal symptoms, and progressive systemic involvement during an outbreak setting. This case highlights the clinical course, diagnostic evaluation, infection control measures, management strategies, and outcome, emphasizing the importance of early recognition, rapid laboratory confirmation, and multidisciplinary supportive care in improving survival.
Introduction
Ebola virus disease is a zoonotic infection caused by enveloped, single-stranded RNA viruses belonging to the family Filoviridae. Since its first identification in 1976, EVD has been associated with multiple outbreaks, most notably the 2014–2016 West African epidemic, which resulted in significant morbidity, mortality, and global public health concern. The disease is transmitted through direct contact with infected body fluids, contaminated surfaces, or infected animals, with healthcare workers being at particularly high risk.
Clinically, EVD is marked by a rapid progression from nonspecific febrile illness to severe gastrointestinal symptoms, hemorrhagic manifestations, shock, and multiorgan failure. Case fatality rates have ranged from 25% to 90%, depending on the outbreak, viral strain, and access to advanced medical care. While no pathognomonic early clinical signs exist, prompt suspicion and diagnosis are critical for patient survival and outbreak containment. This case report describes a typical presentation of EVD and discusses diagnostic challenges, management principles, and prognostic considerations.
Case Report
Patient History
A 29-year-old man presented to an emergency treatment unit in a regional hospital with a 4-day history of high-grade fever, severe fatigue, headache, and myalgia. This was followed by profuse watery diarrhea, vomiting, and abdominal pain over the preceding 48 hours. The patient also reported sore throat and anorexia.
He resided in a rural community experiencing an ongoing Ebola outbreak and reported recent attendance at a funeral for a relative who had died following an undiagnosed febrile illness. There was no prior history of chronic medical illness. The patient had not traveled outside the region and had no known exposure to wild animals.
Clinical Examination
On examination, the patient appeared acutely ill and dehydrated. His temperature was 39.5°C, heart rate 118 beats per minute, blood pressure 90/60 mmHg, and respiratory rate 24 breaths per minute. Oxygen saturation was 96% on room air.
Physical examination revealed conjunctival injection, dry mucous membranes, and diffuse abdominal tenderness without guarding or organomegaly. There was no rash or overt bleeding at presentation. Neurological examination was unremarkable, and there were no signs of meningeal irritation.
Given the epidemiological risk and clinical presentation, the patient was immediately isolated, and barrier nursing protocols were initiated.
Clinical Evaluation
Differential Diagnosis
The initial differential diagnoses included:
• Ebola virus disease
• Severe malaria
• Typhoid fever
• Lassa fever
• Viral hepatitis
• Septicemia
The combination of epidemiological exposure, gastrointestinal symptoms, and rapid clinical deterioration raised a high index of suspicion for EVD.
Investigations
Laboratory Studies
Initial laboratory investigations revealed leukopenia, thrombocytopenia, and elevated liver transaminases, with aspartate aminotransferase levels exceeding alanine aminotransferase. Serum creatinine was mildly elevated, consistent with dehydration and early renal involvement. Coagulation studies showed prolonged prothrombin time.
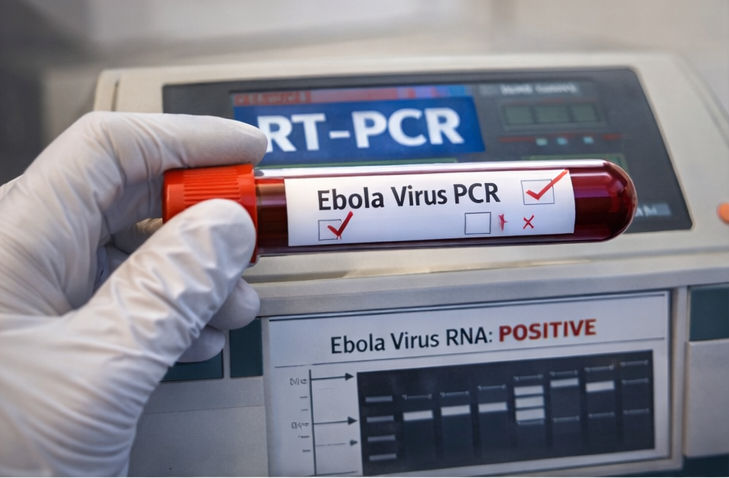
A real-time reverse transcription polymerase chain reaction (RT-PCR) assay for Ebola virus RNA performed on a blood sample returned positive, confirming the diagnosis. Thick and thin blood smears for malaria were negative, and blood cultures showed no bacterial growth.
Diagnosis
Based on clinical presentation, epidemiological exposure, and laboratory confirmation by RT-PCR, a definitive diagnosis of Ebola virus disease was established.
Management and Outcome
Management Strategy
The patient was managed in a dedicated Ebola treatment unit with strict infection prevention and control measures. Supportive care formed the cornerstone of management and included aggressive intravenous fluid resuscitation, electrolyte correction, antipyretics, antiemetics, and nutritional support.
Broad-spectrum antibiotics were initiated empirically to cover possible secondary bacterial infections. Close monitoring of vital signs, urine output, and laboratory parameters was maintained.

The patient was enrolled under an emergency use protocol for an investigational monoclonal antibody-based antiviral therapy, administered according to national treatment guidelines. Blood products were kept on standby in anticipation of potential hemorrhagic complications, although none occurred during the hospital course.

Follow-Up and Outcome
Over the subsequent 10 days, the patient showed gradual clinical improvement. Fever subsided by day 7 of hospitalization, gastrointestinal symptoms resolved, and laboratory parameters demonstrated recovery of platelet counts and liver function.
Repeat RT-PCR testing on days 14 and 16 after symptom onset was negative for Ebola virus RNA. The patient was discharged after 18 days of hospitalization following two consecutive negative tests, in accordance with public health protocols.
At a 1-month follow-up visit, the patient reported persistent fatigue but no neurological or visual symptoms. He was counseled regarding post-Ebola syndrome and advised regular follow-up.
Discussion
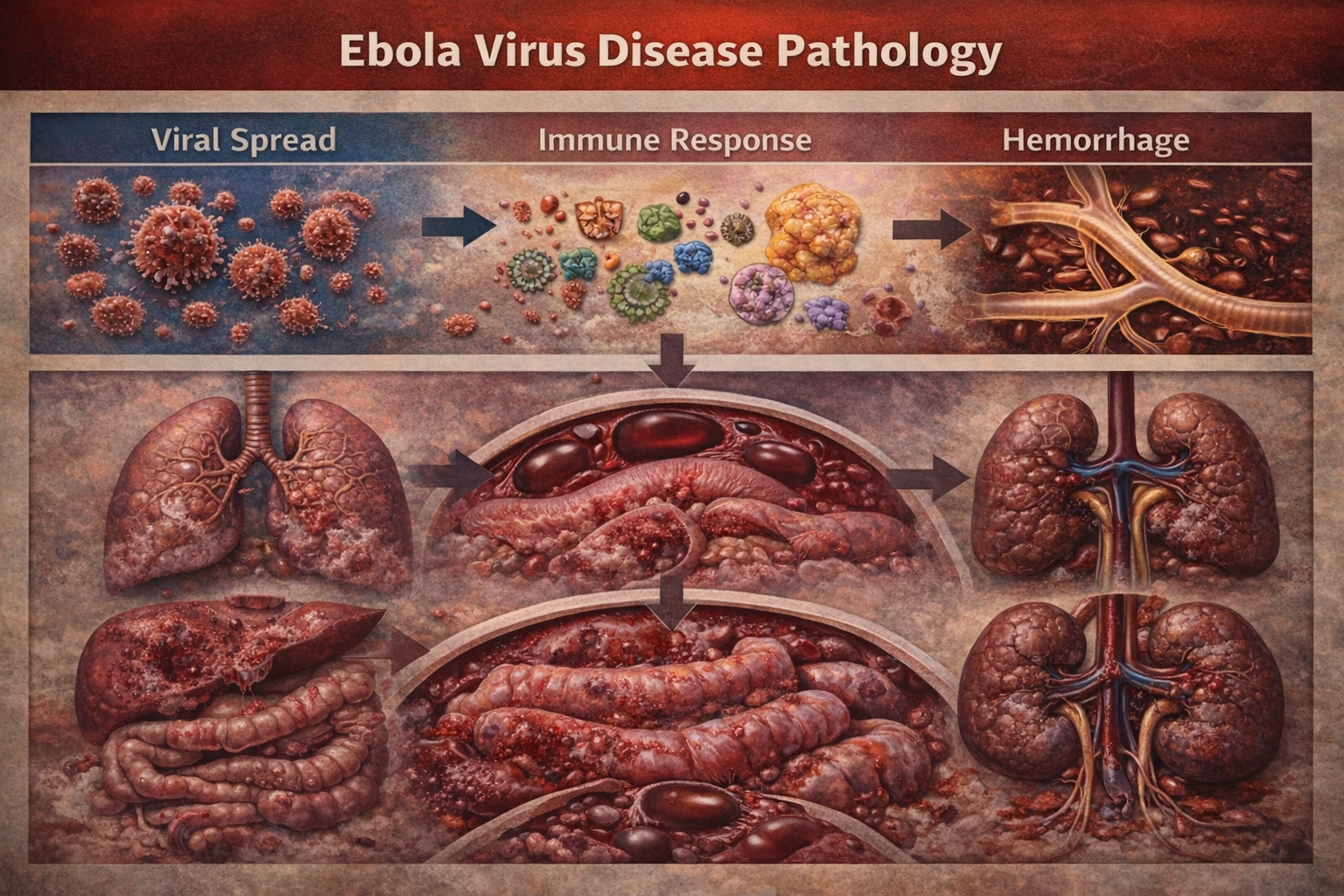
Ebola virus disease remains one of the most lethal infectious diseases known, with pathogenesis driven by widespread viral replication, immune dysregulation, endothelial damage, and coagulopathy. Early symptoms are nonspecific, often mimicking common tropical infections, which contributes to delayed diagnosis and increased transmission risk.
This case underscores the importance of epidemiological context in raising clinical suspicion. Laboratory confirmation using RT-PCR remains the gold standard for diagnosis. Typical laboratory findings include leukopenia, thrombocytopenia, elevated transaminases, and coagulation abnormalities, all of which were observed in this patient.
Supportive care has been shown to significantly reduce mortality, particularly when initiated early. Advances in antiviral and monoclonal antibody therapies have further improved outcomes in recent outbreaks. Survivors may experience long-term sequelae, including fatigue, arthralgia, ocular complications, and neurocognitive symptoms, necessitating structured follow-up care.
Infection control remains paramount, as healthcare-associated transmission has played a significant role in past outbreaks. Strict adherence to personal protective equipment and isolation protocols is essential to protect healthcare workers and limit spread.
Conclusion
Ebola virus disease is a rapidly progressive, life-threatening infection requiring early recognition, prompt isolation, and intensive supportive management. This case illustrates the typical clinical course of EVD and highlights the critical role of epidemiological awareness, molecular diagnostics, and multidisciplinary care in improving patient outcomes. Continued investment in outbreak preparedness, healthcare infrastructure, and access to effective therapeutics is essential to mitigate the global impact of future Ebola outbreaks.
References
-
Feldmann, H., & Geisbert, T. W. (2011). Ebola haemorrhagic fever. The Lancet, 377(9768), 849–862. https://doi.org/10.1016/S0140-6736(10)60667-8
-
World Health Organization. (2023). Ebola virus disease. WHO Fact Sheets. https://www.who.int/news-room/fact-sheets/detail/ebola-virus-disease
-
Kortepeter, M. G., Bausch, D. G., & Bray, M. (2011). Basic clinical and laboratory features of filoviral hemorrhagic fever. Journal of Infectious Diseases, 204(Suppl 3), S810–S816. https://doi.org/10.1093/infdis/jir299
-
Uyeki, T. M., Mehta, A. K., Davey, R. T., et al. (2016). Clinical management of Ebola virus disease in the United States and Europe. New England Journal of Medicine, 374(7), 636–646. https://doi.org/10.1056/NEJMra1504874
-
Sissoko, D., Laouenan, C., Folkesson, E., et al. (2016). Experimental treatment with favipiravir for Ebola virus disease (the JIKI Trial). PLoS Medicine, 13(3), e1001967. https://doi.org/10.1371/journal.pmed.1001967
-
Mulangu, S., Dodd, L. E., Davey, R. T., et al. (2019). A randomized, controlled trial of Ebola virus disease therapeutics. New England Journal of Medicine, 381(24), 2293–2303. https://doi.org/10.1056/NEJMoa1910993
-
Chertow, D. S., Kleine, C., Edwards, J. K., Scaini, R., Giuliani, R., & Sprecher, A. (2014). Ebola virus disease in West Africa—clinical manifestations and management. New England Journal of Medicine, 371(22), 2054–2057. https://doi.org/10.1056/NEJMp1413084
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Year in Review: Chronic Lymphocytic Leukemia
2.
According to a study, white Americans are overdiagnosing melanoma at an alarming rate.
3.
Approval in Endometrial Cancer Expanded; Masks at Cancer Centers; NPR Reporter Dies
4.
The First Gene Therapy Provides a Durable Response for Non-Muscle-Invasive Bladder Cancer.
5.
Canine Cancer Vaccine: A Potential Resurrection? U.S. KK. Snubs Enertu.
1.
What Is Carboxyhemoglobin And How Can It Affect Your Health?
2.
Lu-177 Vipivotide in Prostate Cancer: A Breakthrough in Radioligand Therapy
3.
Unraveling the Mysteries of Coagulopathy: A Comprehensive Definition
4.
Machine Learning in Genomic Analysis for Early Lung Cancer Detection: Key Advances and Insights
5.
A New Perspective on Spherocytosis: Uncovering Innovative Treatments
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Revolutionizing Treatment of ALK Rearranged NSCLC with Lorlatinib - Part II
2.
Navigating the Complexities of Ph Negative ALL - Part XIII
3.
Updates on the First Line Management of ALK+ NSCLC
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
Breaking Ground: ALK-Positive Lung Cancer Front-Line Management - Part II

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge