Tinea Versicolor: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Tinea versicolor is a common superficial fungal infection of the skin caused by lipophilic yeasts of the genus Malassezia. It is characterized by hypo- or hyperpigmented macules and patches, most frequently involving the trunk and proximal extremities. The condition arises due to overgrowth of commensal yeast under favorable conditions such as increased humidity, excessive sweating, seborrheic skin, and altered immune or hormonal states. Although clinically benign and non-contagious, tinea versicolor often leads to cosmetic concern, psychological distress, and frequent recurrence if inadequately treated. Diagnosis is primarily clinical and can be supported by potassium hydroxide (KOH) microscopy, Wood’s lamp examination, and dermoscopic findings. Management predominantly involves topical antifungal agents, while systemic therapy is reserved for extensive, recurrent, or refractory cases. This case report describes an adult patient with classic tinea versicolor, emphasizing clinical features, diagnostic evaluation, therapeutic approach, and short-term outcomes. Early recognition, appropriate antifungal therapy, and patient education are essential for effective disease control and prevention of recurrence.
Introduction
Tinea versicolor, also referred to as pityriasis versicolor, is a superficial mycosis caused by Malassezia species, which are part of the normal cutaneous microbiota. Under certain predisposing conditions, these organisms shift from a harmless yeast form to a pathogenic mycelial form, resulting in clinical disease. The condition is particularly prevalent in tropical and subtropical regions, where high temperature and humidity favor fungal proliferation. Adolescents and young adults are most commonly affected, although the disease may occur at any age.
Several factors predispose individuals to tinea versicolor, including excessive sweating, humid climate, oily skin, use of occlusive clothing, corticosteroid therapy, pregnancy, malnutrition, and immunosuppression. Clinically, the disease presents as well-defined macules and patches that may be hypopigmented, hyperpigmented, or erythematous, often accompanied by fine scaling. Despite being asymptomatic in most cases, the pigmentary alterations can be distressing, particularly in visible areas, leading patients to seek medical attention.
While tinea versicolor is generally easy to diagnose and treat, recurrence is common, especially in predisposed individuals. Awareness of its clinical features, diagnostic modalities, and appropriate management strategies is essential for optimal patient outcomes.
Case Report
Patient History
A 26-year-old male presented to the dermatology outpatient department with a three-month history of asymptomatic discoloration over the upper chest and back.
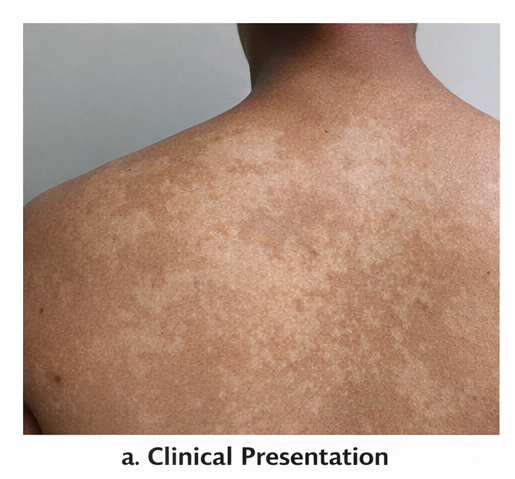
The lesions initially appeared as small patches and gradually increased in size and number. The patient noticed that the discoloration became more prominent following sun exposure, prompting concern. There was no associated pruritus, pain, burning sensation, or systemic symptoms such as fever or weight loss.
The patient reported excessive sweating due to regular outdoor activity and physical exertion. There was no history of diabetes mellitus, immunosuppressive disorders, prolonged medication use, or similar lesions in family members. He had not used any topical or systemic treatment prior to presentation.
Clinical Examination
On cutaneous examination, multiple well-defined hypopigmented and light brown macules and patches were observed over the upper chest, shoulders, and upper back. The lesions varied in size and showed fine, branny scaling, which became more apparent on gentle scraping, demonstrating a positive evoked scale sign. The margins were irregular but well demarcated, and there was no evidence of erythema or inflammation.
Examination of the scalp, face, nails, and mucous membranes was unremarkable. There was no lymphadenopathy or evidence of systemic involvement. Based on the clinical findings, a provisional diagnosis of tinea versicolor was considered.
Clinical Evaluation
Differential Diagnosis
The differential diagnosis for hypopigmented or hyperpigmented macules on the trunk includes:
-
Tinea versicolor
-
Pityriasis alba
-
Seborrheic dermatitis
-
Vitiligo
-
Post-inflammatory hypopigmentation
Careful clinical examination and targeted investigations were performed to establish a definitive diagnosis.
Investigations
-
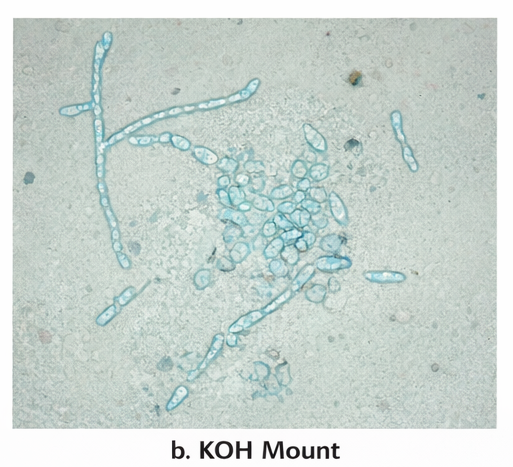
Potassium hydroxide (KOH) mount: Skin scrapings examined under microscopy revealed clusters of short hyphae and round spores in the classic “spaghetti and meatballs” pattern, confirming fungal etiology.
-
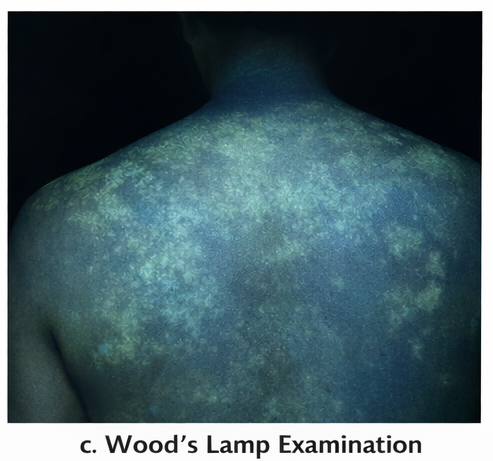
Wood’s lamp examination: A yellowish-green fluorescence was noted over the affected areas, supporting the diagnosis.
-
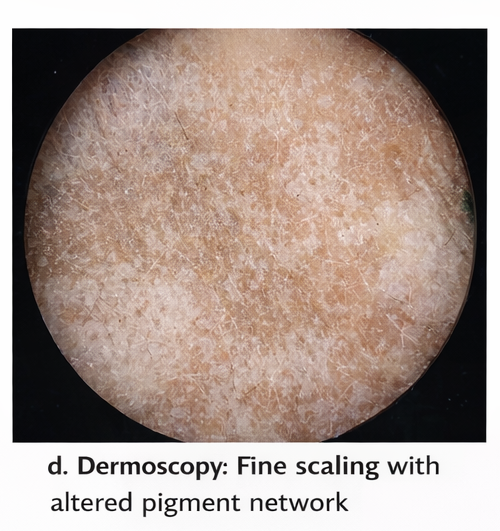
Dermoscopic evaluation: Showed fine scaling and altered pigment network without complete pigment loss.
The collective findings were diagnostic of tinea versicolor.
Management and Outcome
Management Strategy
The patient was managed on an outpatient basis, given the localized nature of the disease and absence of systemic involvement.
Topical therapy included:
-
Ketoconazole 2% shampoo applied to affected areas once daily for five consecutive days, allowing contact for 5–10 minutes before rinsing
-
Ketoconazole 2% cream applied twice daily for two weeks
Adjunctive measures included:
-
Counseling on maintaining proper skin hygiene
-
Avoidance of excessive sweating and tight or occlusive clothing
-
Use of breathable fabrics during hot weather
-
Education regarding the recurrent nature of the disease and the importance of adherence to therapy
Systemic antifungal therapy was not initiated, as the disease was not extensive or refractory.
Follow-Up and Outcome
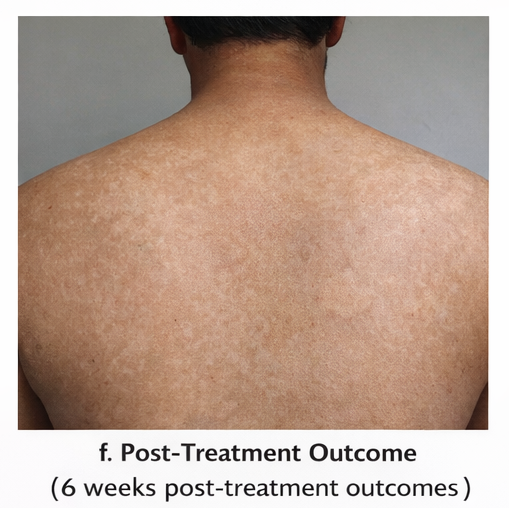
At the two-week follow-up visit, the patient showed complete resolution of scaling, with no progression or appearance of new lesions.

At six weeks, there was noticeable improvement in pigmentation, although mild residual hypopigmentation persisted. This was explained as post-infectious dyspigmentation rather than active disease.
The patient remained asymptomatic and satisfied with the outcome. To reduce the risk of recurrence, monthly prophylactic use of antifungal shampoo during the summer months was advised. The patient was reassured regarding the benign nature of the condition and informed that pigmentary normalization may take several weeks to months.
Discussion
Tinea versicolor is one of the most common superficial fungal infections encountered in dermatological practice. The disease results from altered interaction between Malassezia species and the host skin environment. The organism produces dicarboxylic acids, such as azelaic acid, which interfere with melanocyte function and melanin synthesis, leading to characteristic pigmentary changes.
Diagnosis is often clinical, especially in classic presentations. KOH microscopy remains a simple, rapid, and cost-effective diagnostic tool. Wood’s lamp examination and dermoscopy serve as useful adjuncts, particularly in atypical or early cases. Histopathology is rarely required.
Topical antifungals are the mainstay of treatment and are effective in the majority of patients. Azole antifungals, selenium sulfide, and ciclopirox are commonly used agents. Systemic antifungals, such as itraconazole or fluconazole, are reserved for extensive disease, frequent recurrences, or failure of topical therapy.
A key challenge in managing tinea versicolor is recurrence, which can occur despite adequate treatment. Preventive strategies, including intermittent prophylactic antifungal use and lifestyle modifications, are crucial. Persistence of pigmentary changes after fungal clearance is common and should not be mistaken for treatment failure, as repigmentation may take several months.
Conclusion
Tinea versicolor is a benign but frequently recurrent superficial fungal infection that can cause considerable cosmetic concern. Early clinical recognition, confirmation with simple bedside investigations, and appropriate antifungal therapy result in excellent outcomes. Topical antifungals remain the cornerstone of treatment, while patient education and maintenance strategies play a critical role in preventing recurrence. Awareness of post-treatment pigmentary persistence is essential to avoid unnecessary retreatment and to provide effective patient reassurance.
References
-
The Lancet – Superficial fungal infections: Epidemiology and management
-
Journal of the American Academy of Dermatology – Clinical features and treatment of tinea versicolor
-
British Journal of Dermatology – Diagnostic methods in superficial mycoses
-
Indian Journal of Dermatology – Management guidelines for pityriasis versicolor
-
Cochrane Database of Systematic Reviews – Topical and systemic antifungal therapies for tinea versicolor
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Examines Office-Based Transperineal Prostate Biopsies Methodology.
2.
A global study demonstrates that screening for lung cancer significantly raises the long-term survival rate.
3.
Is a $2,000 Whole-Body MRI Worth It?
4.
Surgery may not be necessary to treat invasive breast cancer
5.
Limited Benefit from New Drugs; Significant Increase in Drug Prices; AI Boost for Mammo Results.
1.
Understanding Evans Syndrome: Causes, Symptoms, and Treatment Options
2.
Understanding Sepsis and Precision-Medicine-Based Immunotherapy: A Pathophysiological Perspective
3.
Exploring The Science Of Hematopoietic Stem Cell Transplantation: What You Need To Know
4.
Unlocking the Secret to Accurate ANC Calculation with This Informative Blog Post
5.
Understanding Lymphedema: Symptoms, Causes, and Treatment
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Pazopanib: A Game-Changer in Managing Advanced Renal Cell Carcinoma - Part VI
2.
Rates of CR/CRi and MRD Negativity in Iontuzumab-Treated Patients
3.
Management of 1st line ALK+ mNSCLC (CROWN TRIAL Update) - Part II
4.
First-Line Maintenance Therapy for Metastatic Urothelial Carcinoma: Bridging Clinical Practice and Trials
5.
Recent Data Analysis for First-Line Treatment of ALK+ NSCLC: A Final Discussion

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge