Umbilical Hernia: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Umbilical hernia is a common abdominal wall defect characterized by the protrusion of intra-abdominal contents through a weakness in the umbilical ring. It is frequently observed in infants and adults, with higher prevalence in individuals with increased intra-abdominal pressure such as obesity, pregnancy, and chronic cough. Although often asymptomatic, umbilical hernias may present with pain, swelling, or complications such as incarceration and strangulation, which require urgent intervention.
We report the case of a 45-year-old female presenting with a progressively enlarging swelling at the umbilicus associated with intermittent pain. Clinical examination and imaging confirmed the diagnosis of an uncomplicated umbilical hernia. The patient underwent elective surgical repair with mesh reinforcement, resulting in excellent postoperative recovery and no recurrence at follow-up.
This case highlights the importance of early diagnosis, appropriate surgical management, and risk factor modification in preventing complications associated with umbilical hernia.
Introduction
Umbilical hernia is defined as a protrusion of abdominal contents through a defect in the umbilical ring. It is a common condition encountered in surgical practice, accounting for a significant proportion of anterior abdominal wall hernias. While congenital umbilical hernias are common in infants and often resolve spontaneously, adult umbilical hernias are typically acquired and require surgical intervention.
The condition arises due to a weakness in the abdominal wall at the umbilicus, which may be exacerbated by increased intra-abdominal pressure. Common etiological factors include obesity, multiparity, ascites, chronic cough, and heavy lifting. The prevalence of umbilical hernia in adults is estimated to be higher in women, particularly those with a history of multiple pregnancies.
Pathophysiologically, the defect allows preperitoneal fat, omentum, or bowel loops to herniate through the fascial opening. Over time, the hernia may enlarge and become symptomatic. Complications such as incarceration (non-reducible hernia) and strangulation (compromised blood supply) can occur, leading to ischemia and requiring emergency surgical intervention.
Risk factors for umbilical hernia include:
• Obesity
• Multiple pregnancies
• Chronic cough or respiratory disease
• Ascites (commonly in liver disease)
• Heavy physical activity
• Previous abdominal surgeries
Clinical presentation varies from an asymptomatic swelling to acute abdomen in complicated cases. Early recognition and timely management are essential to prevent morbidity.
Case Report
Patient History
A 45-year-old female presented to the surgical outpatient department with complaints of:
• Swelling at the umbilical region for 1 year
• Gradual increase in size of the swelling
• Intermittent dull aching pain, aggravated by exertion
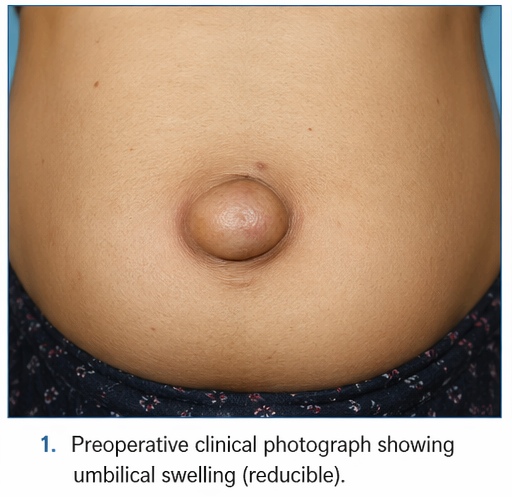
The swelling was initially small and reducible but had progressively increased in size. The patient reported discomfort while standing for prolonged periods and during physical activity.
She had a history of three full-term pregnancies and was overweight (BMI: 29 kg/m²). There was no history of abdominal surgery, trauma, or chronic illness. She denied symptoms such as vomiting, constipation, or signs suggestive of bowel obstruction.
Clinical Examination
On general examination:
• Vital signs were stable
• No signs of systemic illness
Abdominal examination revealed:
• A soft, non-tender swelling at the umbilicus measuring approximately 4 × 3 cm
• The swelling was reducible on gentle pressure
• Positive cough impulse
• No overlying skin changes
There were no signs of incarceration or strangulation. The rest of the abdominal examination was unremarkable.
Clinical Evaluation
Differential Diagnosis
Based on the clinical findings, the following conditions were considered:
• Umbilical hernia
• Paraumbilical hernia
• Epigastric hernia
• Lipoma of the abdominal wall
• Umbilical granuloma
The presence of a reducible swelling with a cough impulse strongly suggested an umbilical hernia.
Investigations
Laboratory Findings
• Complete blood count: Within normal limits
• Liver and renal function tests: Normal
• Blood glucose levels: Normal
Imaging Studies
• Ultrasound abdomen revealed:
– Defect in the anterior abdominal wall at the umbilicus
– Herniation of omental fat through the defect
– No bowel involvement
– No signs of obstruction or strangulation
• CT scan (if performed) may further delineate the size of the defect and contents of the hernia sac, although not required in uncomplicated cases.
Diagnosis
Based on clinical examination and imaging findings, a diagnosis of uncomplicated umbilical hernia was established.
Management and Outcome
Management Strategy
Given the symptomatic nature of the hernia and the risk of future complications, elective surgical repair was planned. A multidisciplinary approach involving surgical and anesthetic teams was adopted.
Surgical Treatment
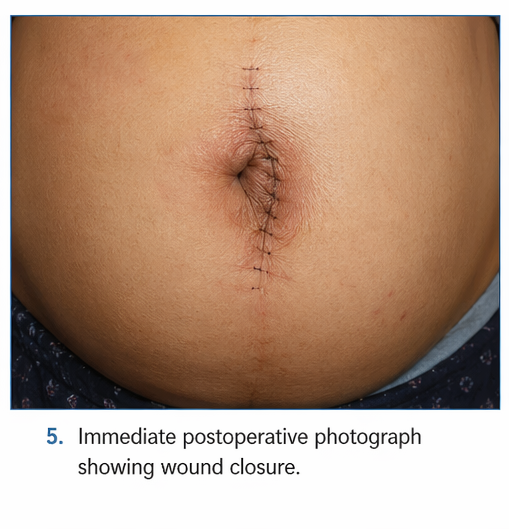
The patient underwent open mesh hernioplasty, which is considered the standard of care for adult umbilical hernia.
Procedure details:
• A small infraumbilical incision was made
• The hernia sac was identified and dissected
• Contents (omentum) were reduced into the abdominal cavity
• The defect was closed
• A synthetic mesh was placed to reinforce the abdominal wall
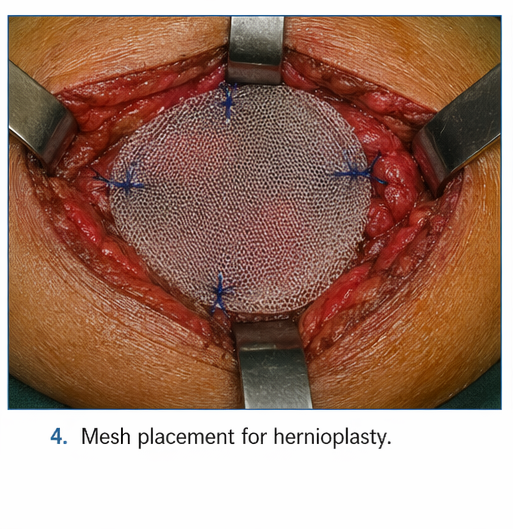
Mesh repair significantly reduces recurrence rates compared to primary suture repair.
Postoperative Care
• Analgesics for pain management
• Early mobilization
• Wound care and infection monitoring
• Advice on avoiding heavy lifting
Follow-Up and Outcome
At 1 week:
• Wound healing was satisfactory
• No signs of infection
At 1 month:
• Complete resolution of symptoms
• No recurrence
At 6 months:
• Patient remained asymptomatic
• No evidence of hernia recurrence
The patient demonstrated excellent recovery with improved quality of life.
Discussion
Pathophysiology
Umbilical hernia develops due to a defect in the abdominal wall fascia at the umbilical ring. Increased intra-abdominal pressure leads to gradual protrusion of intra-abdominal contents. In adults, this defect does not close spontaneously and often enlarges over time.
The hernia sac may contain:
• Preperitoneal fat
• Omentum
• Small intestine
Complications arise when the herniated contents become trapped (incarceration) or when blood supply is compromised (strangulation), leading to ischemia and necrosis.
Diagnostic Challenges
Diagnosis is primarily clinical but may be challenging in obese patients or small hernias.
Key challenges include:
• Differentiating from other abdominal wall swellings
• Detecting early complications
• Identifying occult hernias
Imaging modalities such as ultrasound and CT scan are useful adjuncts in uncertain cases.
Treatment Considerations
Surgical Repair
Surgery is the definitive treatment for adult umbilical hernia.
Options include:
• Primary suture repair (for small defects)
• Mesh repair (preferred due to lower recurrence rates)
• Laparoscopic repair (minimally invasive option)
Mesh repair is widely recommended due to its superior outcomes and reduced recurrence.
Indications for Surgery
• Symptomatic hernia
• Increasing size
• Cosmetic concerns
• Risk of complications
Emergency surgery is required in cases of strangulation or bowel obstruction.
Complications
If untreated, umbilical hernia can lead to:
• Incarceration
• Strangulation
• Bowel obstruction
• Ischemia and necrosis
• Peritonitis
Postoperative complications may include:
• Wound infection
• Seroma formation
• Mesh-related complications
• Recurrence
Prognosis
The prognosis of umbilical hernia is generally favorable with timely surgical intervention. Mesh repair has significantly improved outcomes and reduced recurrence rates.
Factors influencing prognosis include:
• Size of hernia defect
• Surgical technique
• Patient comorbidities (e.g., obesity, diabetes)
• Adherence to postoperative care
Conclusion
Umbilical hernia is a common surgical condition that can significantly impact patient quality of life if left untreated. This case highlights the importance of early diagnosis and timely surgical intervention to prevent complications.
Elective mesh repair remains the gold standard for adult umbilical hernia, offering excellent outcomes and low recurrence rates. Patient education regarding lifestyle modification, weight management, and avoidance of risk factors is crucial in preventing recurrence.
A comprehensive, patient-centered approach ensures optimal clinical outcomes and long-term success in the management of umbilical hernia.
References
- Ponten, J. E. H., Thomassen, I., & Nienhuijs, S. W. (2014). A collective review on mesh-based repair of umbilical and epigastric hernias. Indian Journal of Surgery. https://pubmed.ncbi.nlm.nih.gov/26396470/
- Aiolfi, A., Cavalli, M., Micheletto, G., et al. (2020). Open mesh versus suture repair of umbilical hernia: systematic review and trial sequential meta-analysis. Hernia. https://pubmed.ncbi.nlm.nih.gov/32096090/
- Kaufmann, R., Halm, J. A., Eker, H. H., et al. (2018). Mesh versus suture repair of umbilical hernia in adults: a randomized controlled trial. The Lancet. https://pubmed.ncbi.nlm.nih.gov/29459021/
- Henriksen, N. A., Jensen, K. K., Bisgaard, T., & Helgstrand, F. (2022). Suture or mesh repair of the smallest umbilical hernias: a nationwide database study. World Journal of Surgery. https://pubmed.ncbi.nlm.nih.gov/35306587/
- Moradian, S., Klosowiak, J. L., Boctor, M. J., et al. (2023). Novel approach for umbilical hernia repair using mesh strips. Plastic and Reconstructive Surgery Global Open. https://pubmed.ncbi.nlm.nih.gov/37113310/
- Arroyo, A., García, P., Pérez, F., et al. (2001). Randomized clinical trial comparing suture and mesh repair of umbilical hernia in adults. British Journal of Surgery. https://pubmed.ncbi.nlm.nih.gov/11578208/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge