Aplasia Cutis Congenita in a Newborn Following Maternal Methimazole Exposure: A Case Report
OthersPage Navigation
Abstract
Aplasia cutis congenita (ACC) is a rare congenital disorder characterized by focal absence of skin at birth, most commonly involving the scalp [1,2]. Several etiological factors have been implicated, including genetic predisposition, vascular compromise, intrauterine infections, and teratogenic drug exposure [1,3]. We report a case of scalp aplasia cutis congenita in a newborn born to a mother who received methimazole during early pregnancy. Maternal exposure to methimazole is a well-recognized risk factor and forms part of the methimazole embryopathy spectrum [4,5]. Early recognition and conservative management resulted in favorable clinical outcomes.
Introduction
Aplasia cutis congenita is defined as a congenital absence of skin, which may involve only the epidermis or extend to deeper structures such as the dermis, subcutaneous tissue, bone, or dura mater [1,2]. The condition has an estimated incidence of 1–3 per 10,000 live births and most frequently affects the scalp, particularly the vertex region [2,6].
The etiology of ACC is heterogeneous and includes genetic factors, placental insufficiency, amniotic band disruption, intrauterine infections, and exposure to teratogenic medications during pregnancy [1,3]. Among drug-related causes, antithyroid medications—especially methimazole—have been strongly associated with congenital anomalies, including aplasia cutis congenita, choanal atresia, and esophageal atresia [4,5]. Methimazole crosses the placenta and interferes with fetal development, particularly when exposure occurs during the first trimester [4,7].
.png)
Case Report
Maternal History
A 28-year-old primigravida with a known diagnosis of Graves’ disease was treated with methimazole during the antenatal period, including the first trimester of pregnancy, which is a critical window for fetal organogenesis [4,5]. Methimazole use in early pregnancy has been associated with a higher risk of congenital anomalies when compared with alternative antithyroid drugs, particularly propylthiouracil, due to its recognized teratogenic potential during this stage of development [4,7]. The mother remained clinically euthyroid during most of the pregnancy, and antenatal follow-up visits were regular. There was no history of maternal infections, diabetes mellitus, hypertension, radiation exposure, or use of other known teratogenic medications during pregnancy [3]. The pregnancy was otherwise uneventful, with normal routine antenatal investigations and ultrasound findings. Family history was non-contributory, with no reported congenital anomalies, genetic disorders, or similar dermatological conditions among close relatives..
Neonatal Presentation
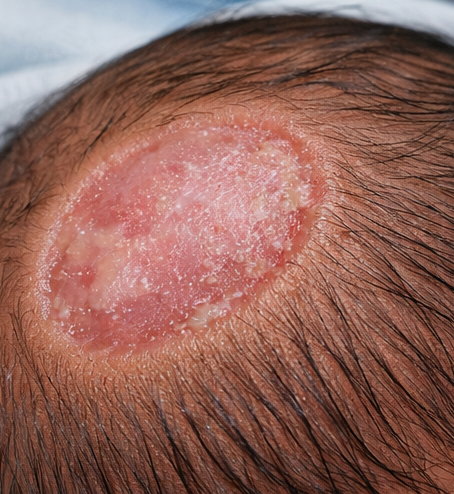
A term male neonate was delivered via normal vaginal delivery with normal Apgar scores at one and five minutes, indicating good immediate postnatal adaptation. At birth, a well-defined scalp defect was noted over the vertex region, which is consistent with the most common site of involvement in aplasia cutis congenita [2,6].

The lesion measured approximately a few centimeters in diameter and was clearly demarcated from the surrounding normal skin. It was painless, non-inflammatory, and covered by a thin, translucent membrane, with no evidence of active bleeding, ulceration, or purulent discharge, features that are characteristic of superficial ACC lesions [1,2].

The surrounding scalp appeared healthy, with no erythema, induration, or signs of secondary infection. A thorough head-to-toe examination revealed no additional cutaneous abnormalities, dysmorphic features, or congenital malformations involving other organ systems. Neurological examination was normal, and the infant exhibited normal tone, reflexes, and feeding behavior, further supporting the absence of associated anomalies.
Clinical Findings
Cutaneous examination revealed a solitary, oval area of absent skin measuring approximately 3 × 2 cm, with sharply demarcated margins and absence of hair over the lesion [1,6]. The surrounding skin was normal, and there were no signs of infection, inflammation, or ulceration, which is typical of isolated ACC [2,3]. Neurological and systemic examinations were unremarkable, supporting the absence of deeper or syndromic involvement [6].
Investigations
Routine laboratory investigations were within normal limits. Cranial ultrasonography demonstrated intact underlying bone and no intracranial abnormalities, which is recommended to exclude skull or dural involvement in scalp ACC [2,3]. Based on clinical findings and maternal history of methimazole exposure, a diagnosis of methimazole-associated aplasia cutis congenita was made [4,5].
Discussion
Aplasia cutis congenita commonly presents as a painless, well-circumscribed defect at birth, most frequently involving the scalp, particularly the vertex region, which accounts for the majority of reported cases [1,2]. The lesions may vary in size and depth, ranging from superficial absence of epidermis to deeper involvement of the dermis, subcutaneous tissue, and, in rare cases, underlying bone or dura mater [2,3]. Because ACC lesions are often non-tender and lack overt inflammatory signs, affected infants usually appear otherwise healthy at birth. In cases where lesions are small or located in less visible areas, the absence of systemic symptoms may result in delayed recognition and diagnosis [6]. In contrast, scalp lesions are typically identified immediately after delivery due to their conspicuous location and characteristic appearance [1,6].
Methimazole exposure during early pregnancy has been consistently linked to ACC as part of a broader methimazole embryopathy syndrome, which may also include choanal atresia, esophageal atresia, facial dysmorphism, and developmental anomalies [4,5]. The teratogenic effect of methimazole is believed to result from interference with embryonic tissue differentiation, impaired angiogenesis, and disruption of thyroid hormone–dependent developmental pathways during critical stages of organogenesis [3,7]. These effects are most pronounced when exposure occurs during the first trimester, a period of rapid fetal growth and morphogenesis. Compared with propylthiouracil, methimazole has been shown to carry a higher risk of congenital malformations when used in early pregnancy, leading current guidelines to recommend careful drug selection and close monitoring in women of reproductive age with hyperthyroidism [4,7].
Management
Management of aplasia cutis congenita is guided primarily by lesion size, depth, and the presence or absence of associated anomalies. Small, superficial lesions without bone involvement are best managed conservatively, with meticulous local wound care, protection from trauma, and prevention of secondary infection [2,3]. Larger or deeper defects may require surgical intervention to reduce the risk of complications such as hemorrhage, infection, or sagittal sinus exposure [2]. Early diagnosis and timely, appropriate management, as demonstrated in this case, are associated with excellent outcomes, minimal long-term morbidity, and satisfactory cosmetic results [1,6].

Conclusion
Aplasia cutis congenita should be suspected in newborns presenting with localized absence of skin, particularly when the defect involves the scalp, which is the most commonly affected site [1,2]. The characteristic appearance of a well-demarcated, non-inflammatory lesion at birth should prompt clinicians to consider ACC in the differential diagnosis and initiate further evaluation. Careful clinical assessment is essential to determine the size, depth, and extent of the lesion, as these factors influence both management and prognosis [2,3].
A detailed maternal history, with specific emphasis on medication exposure during pregnancy, is a critical component of evaluation, as antenatal methimazole use is a well-established risk factor for the development of ACC [4,5]. Inquiry regarding the timing, dosage, and duration of antithyroid drug therapy is particularly important, as first-trimester exposure carries the greatest teratogenic risk. In addition to medication history, clinicians should assess for other potential contributing factors, including maternal infections, placental abnormalities, and family history of congenital anomalies [3].
Early recognition of ACC allows for timely investigations, including imaging studies such as cranial ultrasonography or magnetic resonance imaging, to exclude underlying skull or dural defects and to assess the risk of associated complications [2]. Prompt identification also facilitates appropriate management planning, which in many cases involves conservative measures such as local wound care, infection prevention, and close follow-up [3]. With early diagnosis and appropriate intervention, most infants with isolated, superficial ACC experience favorable outcomes with minimal long-term morbidity.
Increased awareness among obstetricians, neonatologists, pediatricians, and dermatologists regarding drug-related causes of ACC is essential for both prevention and early diagnosis [3,7]. Such awareness supports informed decision-making when prescribing medications to women of childbearing age, enhances prenatal counseling, and enables effective parental education and reassurance following diagnosis, ultimately improving overall clinical outcomes.
References
- Frieden IJ. Aplasia cutis congenita: A clinical review and proposal for classification. J Am Acad Dermatol. 1986;14(4):646–660.
- Sybert VP. Aplasia cutis congenita: A report of 12 new families and review of the literature. Pediatrics. 1985;76(4):594–603.
- Browning JC. Aplasia cutis congenita: Approach to evaluation and management. Dermatol Ther. 2013;26(6):439–444.
- Cooper DS. Antithyroid drugs in pregnancy: Methimazole and congenital anomalies. Endocr Pract. 2009;15(4):330–334.
- Bahn RS, et al. Hyperthyroidism and other causes of thyrotoxicosis: Management guidelines of the American Thyroid Association. Thyroid. 2011;21(6):593–646.
- Martinez-Regueira S, et al. Aplasia cutis congenita: Epidemiologic and clinical features. Pediatr Dermatol. 2006;23(6):537–541.
- Di Gianantonio E, et al. Methimazole embryopathy: Delineation of the phenotype. Am J Med Genet. 2001;99(3):219–223.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Does pollution cause cancer?
2.
AI is equally capable of reading breast cancer scans as human radiologists.
3.
EVP Beats Cisplatin for Resectable MIBC
4.
New research points out a promising strategy for treating metastatic medulloblastoma
5.
Academics + Pharma = Big Bucks; New CAR-T Warnings; Patients Seek Cancer Tests.
1.
A Closer Look at Breast Cancer: Examining the Ultrasound Images
2.
Unlocking the Secrets of Oral Cancer Staging: A New Approach to Early Detection
3.
Impact of Hormone Therapy Cessation on Tumor Growth: Case Study of Ki-67 Reduction
4.
Unraveling the Mysteries of Lymphoma: A Journey into the Unknown
5.
Refining AML Survival: Prognostic Factors, Therapies, and Stem Cell Strategies Reviewed
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Navigating the Complexities of Ph Negative ALL - Part III
2.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VIII
3.
Management of 1st line ALK+ mNSCLC (CROWN TRIAL Update)
4.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part III
5.
Virtual Case Study on Pedal Edema and Triple Vessel Disease - An Initiative by Hidoc Dr.

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge