Gingival Exostosis: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Gingival exostosis is a benign, localized bony overgrowth projecting from the alveolar bone into the gingival soft tissue. It is usually slow-growing, asymptomatic, and often detected during routine oral examination or when it interferes with oral hygiene. Although benign, it may cause discomfort, esthetic concerns, and difficulties with prosthetic rehabilitation when prominent. Accurate clinical assessment and radiographic imaging are essential to distinguish it from other osseous and soft tissue lesions of the oral cavity. This case report describes an adult patient with gingival exostosis, outlining clinical features, diagnostic approach, management, histopathological findings, and outcomes, with emphasis on differential diagnosis and treatment considerations.
Introduction
Gingival exostosis is a type of benign bony outgrowth that arises from the cortical plate of the alveolar bone and protrudes through the overlying gingiva. It may be solitary or multiple and is more commonly observed on the buccal aspect of the maxilla and, less frequently, the mandible. The condition is more commonly identified in adults and has been variably associated with genetic factors, parafunctional habits, occlusal stress, and chronic low-grade irritation from plaque and calculus.
Though typically asymptomatic, gingival exostoses gain clinical relevance when they cause gingival trauma, impede oral hygiene, or complicate prosthetic device placement. Differential diagnosis includes benign fibro-osseous lesions, osteomas, peripheral ossifying fibromas, and other gingival hyperplastic conditions. Appropriate diagnostic evaluation involves clinical examination, radiographic assessment, and, where indicated, histopathological confirmation. This report presents a case of gingival exostosis affecting the maxillary buccal gingiva in a middle-aged female, illustrating the diagnostic and therapeutic pathway.
Case Report
Patient History
A 45-year-old female presented to the dental outpatient department with a painless swelling on the upper gum of the right side that she had first noticed eight months prior. She reported that the swelling appeared gradually and had increased in size slowly. The patient described occasional discomfort with toothbrushing and minor irritation from cheek friction but denied spontaneous pain, bleeding, ulceration, or discharge.
There was no history of recent dental procedures or trauma. She had no significant medical conditions, was not on regular medication, and had no known drug allergies. She denied smoking or tobacco use. Family history was non-contributory. There were no systemic symptoms such as fever, weight loss, or night sweats.
Clinical Examination
Extraoral examination did not reveal facial asymmetry or lymphadenopathy. Intraoral inspection revealed a solitary, well-defined, firm swelling on the buccal gingiva in the region of the right maxillary first and second premolars.

The lesion measured approximately 1.8 × 1.2 cm, was covered by normal-appearing mucosa, and was non-tender on palpation.
The mass was firm and immobile, suggestive of an osseous origin. There was good oral hygiene, with no significant plaque or calculus accumulation in the region. Periodontal probing around the involved teeth revealed shallow sulcus depths with no evidence of periodontal pockets. Teeth in the region were non-carious and responded normally on vitality testing.
No peripheral stigmata such as ulceration, sinus tracts, or soft tissue tags were present. The patient’s occlusion was Class I with balanced contacts and no signs of parafunctional wear.
Clinical Evaluation
Differential Diagnosis
Based on clinical presentation, the following diagnoses were considered:
-
Gingival exostosis
-
Peripheral ossifying fibroma
-
Peripheral osteoma
-
Fibrous hyperplasia
-
Benign fibro-osseous lesion
The firm, bony consistency of the lesion combined with lack of inflammatory signs and normal overlying mucosa supported the provisional diagnosis of gingival exostosis.
Investigations
Radiographic Evaluation
A standard intraoral periapical (IOPA) radiograph revealed a well-circumscribed radiopaque mass on the buccal aspect of the right maxillary premolar region, continuous with the underlying alveolar bone. There was no evidence of bone destruction, root resorption, periapical pathology, or periodontal bone loss.

Advanced Imaging
To further characterize the bony lesion, a cone-beam computed tomography (CBCT) scan was obtained. The CBCT confirmed an exophytic bony outgrowth arising from the buccal cortical plate, extending into the overlying gingival soft tissues (Figure images not included). The trabecular pattern and continuity with the cortical bone were consistent with a benign osseous growth.
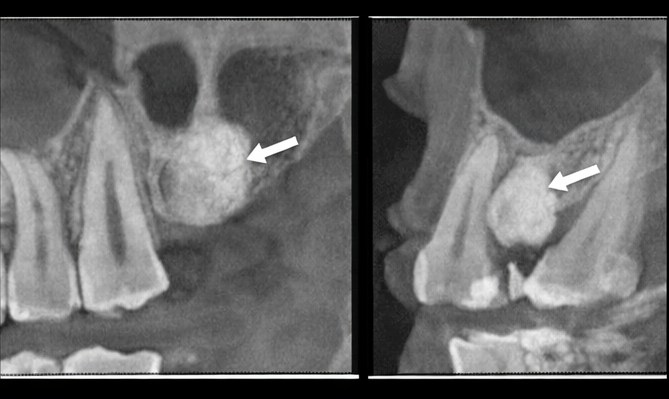
The radiographic findings, along with clinical examination, supported gingival exostosis as the most likely diagnosis.
Management and Outcome
Treatment Planning
Because the lesion was causing mild functional discomfort and had the potential to interfere with future prosthetic planning and hygiene maintenance, surgical excision was recommended.
Surgical Procedure
Under local anesthesia, a crevicular incision was made around the involved teeth, and a mucoperiosteal flap was reflected to expose the bony mass. The exostosis was carefully excised using a round diamond bur and surgical handpiece, ensuring smooth contours of the remaining alveolar bone. Hemostasis was achieved, and the flap was repositioned and sutured with resorbable sutures.
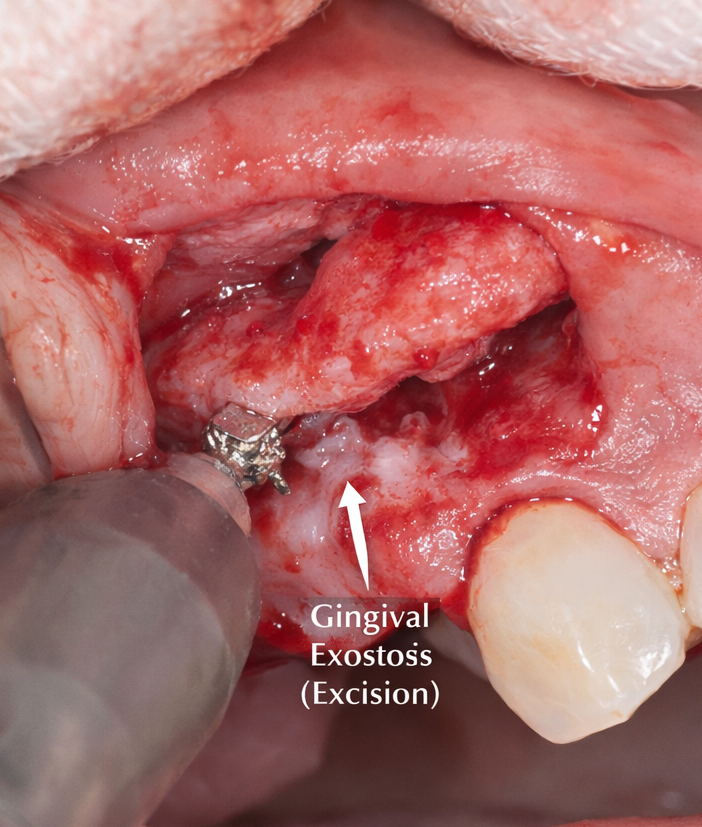
The excised specimen was submitted for histopathological analysis.
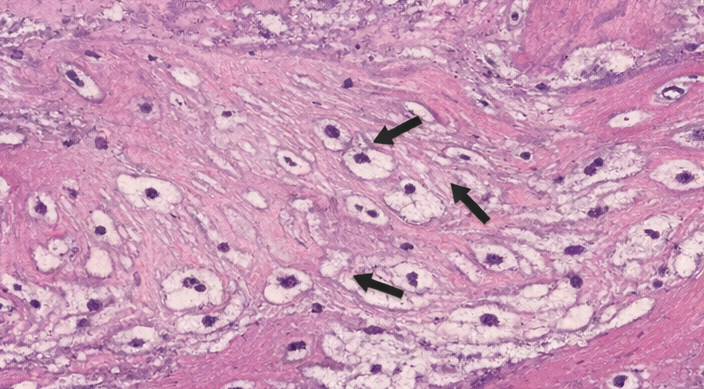
Histopathological Findings
Microscopic examination demonstrated dense lamellar bone with normal-appearing osteocytes in lacunae. Marrow spaces were minimal, and there was no evidence of cellular atypia, inflammation, or malignancy. The histopathological features were consistent with a benign exostotic growth.
Follow-Up and Outcome
The postoperative course was uneventful. The patient was prescribed analgesics and chlorhexidine mouth rinse and advised to avoid trauma to the surgical site. Sutures were removed after one week, and soft tissue healing was progressing well.
At four-week and three-month follow-ups, complete mucosal healing was observed. The patient reported resolution of prior discomfort and expressed satisfaction with the esthetic outcome. There were no signs of recurrence on clinical or radiographic examination at six-month follow-up.
Discussion
Gingival exostoses are benign osseous protuberances that originate from the alveolar bone and are covered by gingival tissues. Although the exact etiology is not fully understood, several factors are implicated, including mechanical stress (e.g., occlusal forces), genetic predisposition, and chronic low-grade irritation. These lesions are typically asymptomatic and slow growing, often discovered incidentally unless they cause irritation or interfere with oral function.
Clinically, gingival exostosis presents as a firm, immobile mass covered by normal mucosa, most commonly on the buccal aspect of the maxilla. Periodontal evaluation and radiographic imaging are essential to differentiate it from other gingival enlargements and benign fibro-osseous lesions. Radiographs typically show a radiopaque outgrowth continuous with the alveolar cortex.
Histopathology remains the gold standard for confirmation and exclusion of neoplastic or fibro-osseous conditions. Complete surgical excision is indicated when the lesion interferes with hygiene, causes patient discomfort, or complicates dental prosthetic planning.
The prognosis following excision is excellent with a low likelihood of recurrence. Long-term follow-up is recommended to monitor for potential regrowth.
Conclusion
Gingival exostosis is a benign alveolar bone overgrowth that may present as a firm, asymptomatic gingival mass. Accurate diagnosis requires careful clinical and radiographic evaluation. Surgical excision offers definitive treatment when lesions cause functional discomfort, interfere with hygiene, or pose challenges for prosthetic planning. Histopathological confirmation is recommended to rule out other fibro-osseous or neoplastic conditions. Long-term prognosis is favorable, with rare recurrence observed following complete excision.
References
- Neville BW, Damm DD, Allen CM, Chi AC. Oral and Maxillofacial Pathology (4th ed.). Elsevier https://www.elsevier.com/books/oral-and-maxillofacial-pathology/neville/978-0-323-35769-2
- Regezi JA, Sciubba JJ, Jordan RC. Oral Pathology: Clinical Pathologic Correlations. Elsevier. https://www.elsevier.com/books/oral-pathology/regezi/978-0-323-52938-9
- Kfir Y, Buchner A, Hansen LS. Reactive lesions of the gingiva. J Periodontol. 1980;51(11):655–661. https://pubmed.ncbi.nlm.nih.gov/6935670/
- Eisenbud L, Stern M, Rothberg M, Sachs SA. Benign osteogenic tumors of the jaws. Oral Surg Oral Med Oral Pathol. 1999;88(5):574–580. https://pubmed.ncbi.nlm.nih.gov/10594891/
- Ongole R, Koneru S, Kumar SA, Kottu R, Siddamsetty V. Buccal exostosis – A review and case report. J Clin Diagn Res. 2015;9(5):ZD10-ZD12. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4475572/
- Gupta M, Srivastava D, Srivastava R, Pradhan D. Exostosis: A clinical review and case report. J Indian Soc Periodontol. 2018;22(2):158-162. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5914761/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Non-Factor Therapies in Hemophilia: Cutting-Edge Approaches to Individualize Care
2.
FDA approves Blenrep for relapsed or refractory multiple myeloma
3.
X-ray and radar technology combined to reduce cancer screening risks
4.
Extended Maintenance with Imatinib Enhances Disease-Free Survival in High-Risk GIST.
5.
Researchers discuss HER2-low and HER2-zero in breast cancer
1.
Understanding Mesenteric Masses: Symptoms, Diagnosis, and Treatment Options
2.
Liposomal Doxorubicin and Mitomycin in Modern Cancer Treatment
3.
The New Era of Oncology: Key Updates and Clinical Insights
4.
HIPEC in Platinum-Sensitive Ovarian Cancer: A Promising Yet Controversial Option
5.
Theranostics and Radioligand Therapy: Precision Cancer Care with Targeted Radionuclides
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Exploring Potentials of Lorlatinib: The Third Generation ALK-TKI Through CROWN Trial
2.
Managing ALK Rearranged Non-Small Cell Lung Cancer with Lorlatinib - Part I
3.
Breaking Ground: ALK-Positive Lung Cancer Front-Line Management - Part V
4.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part II
5.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part III

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge