Breast Cancer Presenting as a Palpable Breast Lump: Clinical Evaluation, Diagnostic Workup, and Multidisciplinary Management - A Case Report
OthersPage Navigation
Abstract
Breast cancer is the most commonly diagnosed malignancy among women worldwide and a leading cause of cancer-related mortality. It is a biologically heterogeneous disease with varied clinical presentations, histopathological subtypes, and molecular profiles, which significantly influence prognosis and therapeutic decision-making. Early detection through clinical examination and imaging plays a critical role in improving survival outcomes.
We report a case of invasive breast carcinoma in a middle-aged woman presenting with a painless breast lump. This case highlights the importance of early clinical suspicion, comprehensive diagnostic evaluation including imaging and histopathology, molecular subtyping, and the role of a multidisciplinary approach in individualized treatment planning and follow-up.
Introduction
Breast cancer represents a major global health burden, accounting for approximately one-quarter of all cancers diagnosed in women. The disease arises from malignant transformation of epithelial cells lining the ducts or lobules of the breast and exhibits wide variability in clinical behavior and treatment response [1].
Risk factors include increasing age, genetic predisposition (such as BRCA1 and BRCA2 mutations), hormonal influences, reproductive history, and lifestyle factors [2]. Advances in imaging, molecular diagnostics, and systemic therapies have substantially improved survival; however, delayed presentation remains a significant challenge in many settings.
This case report describes the clinical presentation, diagnostic pathway, histopathological findings, and multidisciplinary management of a patient with invasive breast carcinoma, emphasizing evidence-based decision-making and coordinated care.
Case Report
Patient History
A 48-year-old woman presented to the surgical outpatient department with a complaint of a painless lump in her left breast, noticed two months prior to presentation. The lump had gradually increased in size and was not associated with nipple discharge, skin changes, or breast pain.
There was no history of fever, trauma, or prior breast disease. The patient had attained menarche at 12 years of age and had two full-term pregnancies, with breastfeeding for both children. She had no history of oral contraceptive use or hormone replacement therapy. There was no known family history of breast or ovarian cancer.
Clinical Examination
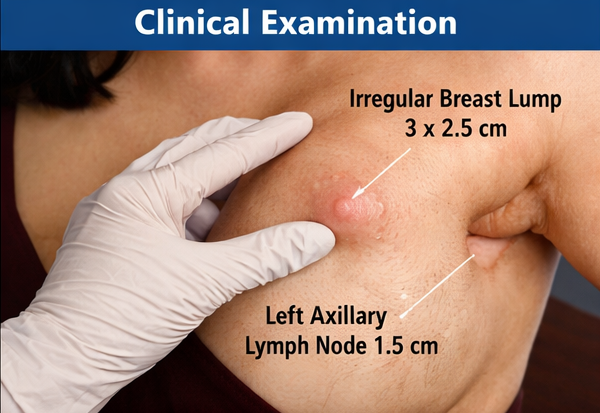
On physical examination, the patient was hemodynamically stable and appeared in good general health. Breast examination revealed a firm, non-tender, irregular mass measuring approximately 3 × 2.5 cm in the upper outer quadrant of the left breast. The mass was poorly mobile with ill-defined margins.
Overlying skin showed mild dimpling, but no erythema or peau d’orange appearance. The nipple-areolar complex was normal. Examination of the left axilla revealed a single, firm, mobile lymph node measuring approximately 1.5 cm. Examination of the contralateral breast and axilla was unremarkable. No hepatosplenomegaly or bony tenderness was noted.
Clinical Evaluation
Initial Differential Diagnosis
Based on clinical findings, the following differential diagnoses were considered:
• Fibroadenoma
• Breast cyst
• Phyllodes tumor
• Invasive breast carcinoma
Given the patient’s age, clinical features, and axillary lymphadenopathy, malignancy was considered the most likely diagnosis.
Investigations
Laboratory Studies
Baseline laboratory investigations, including complete blood count, liver and renal function tests, were within normal limits. Tumor markers were not elevated.
Radiological Evaluation
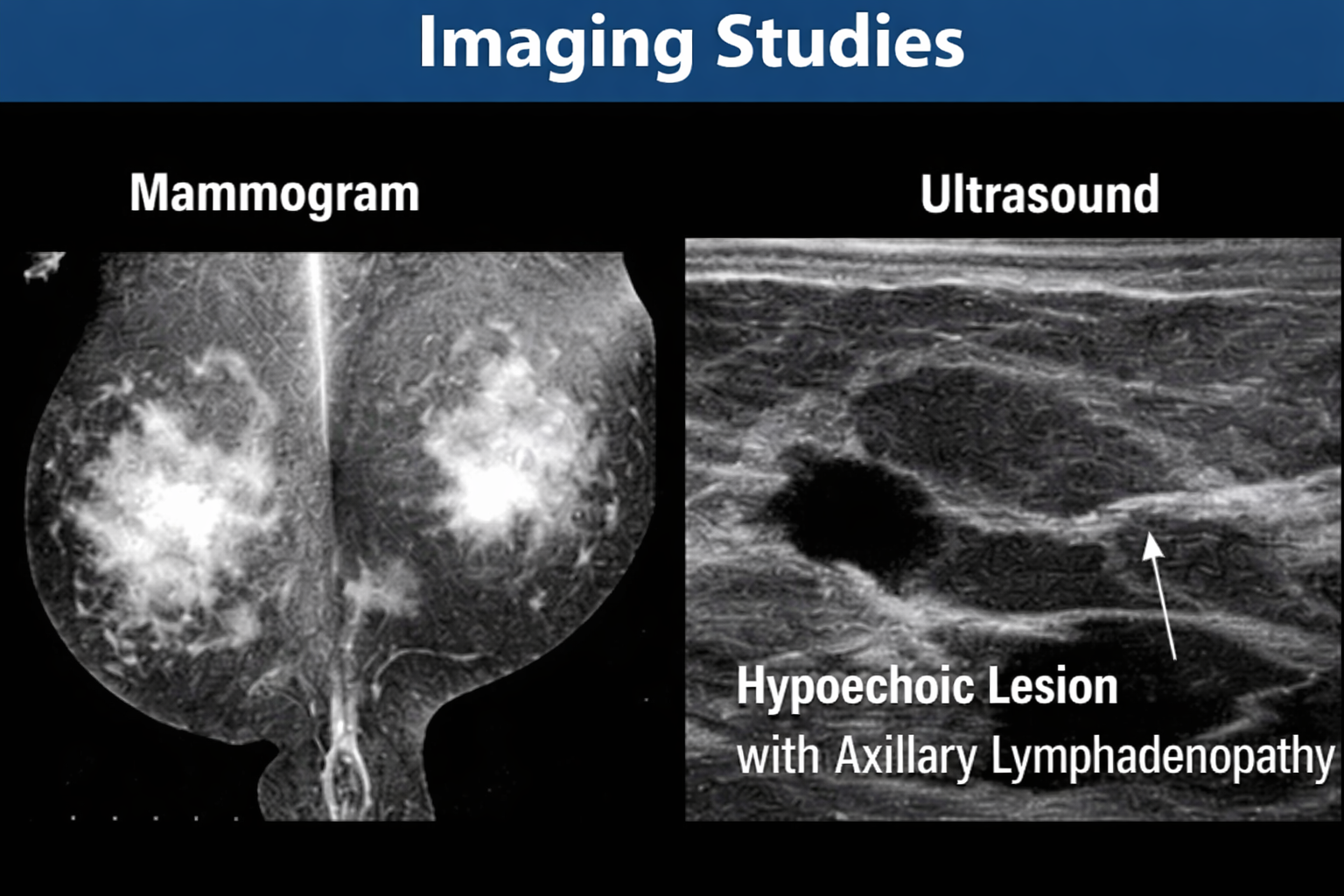
Bilateral mammography demonstrated an irregular, spiculated mass in the upper outer quadrant of the left breast, categorized as BI-RADS 5, highly suggestive of malignancy.
Breast ultrasonography revealed a hypoechoic, irregular lesion with posterior acoustic shadowing and increased vascularity. Enlarged left axillary lymph nodes with cortical thickening were also noted.
Contrast-enhanced computed tomography (CT) of the chest and abdomen showed no evidence of distant metastasis.
Diagnosis
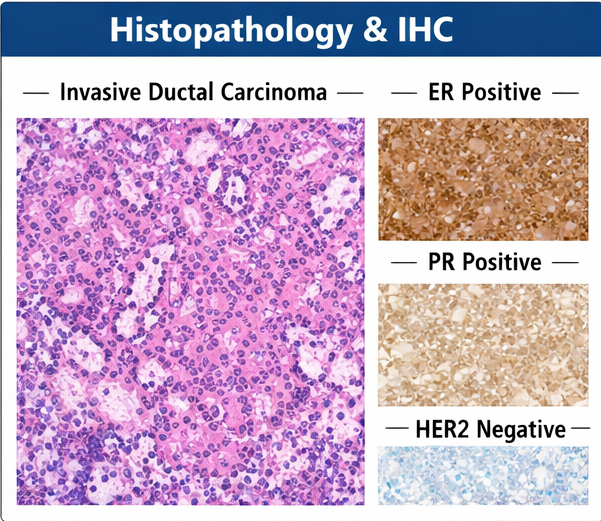
Ultrasound-guided core needle biopsy of the breast lesion revealed invasive ductal carcinoma, not otherwise specified. Histopathological examination showed malignant epithelial cells arranged in nests and cords with moderate nuclear pleomorphism and increased mitotic activity.
Immunohistochemistry demonstrated estrogen receptor (ER) positivity, progesterone receptor (PR) positivity, and human epidermal growth factor receptor 2 (HER2) negativity, consistent with a luminal A molecular subtype.
Based on clinical, radiological, and pathological findings, the patient was diagnosed with stage II (T2N1M0) breast cancer.
Management and Outcome
Multidisciplinary Approach
The case was discussed in a multidisciplinary tumor board comprising surgical oncologists, medical oncologists, radiation oncologists, radiologists, pathologists, and oncology nursing staff. An individualized treatment plan was formulated in accordance with current clinical guidelines.
Therapeutic Management
The patient underwent modified radical mastectomy of the left breast with axillary lymph node dissection. Postoperative recovery was uneventful.
Histopathological examination of the surgical specimen confirmed invasive ductal carcinoma with metastasis in two of the twelve dissected axillary lymph nodes. Surgical margins were free of tumor.

Adjuvant chemotherapy was initiated, followed by adjuvant radiotherapy to the chest wall and regional lymph nodes. Given the hormone receptor–positive status, the patient was started on adjuvant endocrine therapy with tamoxifen.
Follow-Up and Outcome
The patient was followed regularly with clinical examinations and imaging as per protocol. At 12-month follow-up, she remained disease-free with no evidence of local recurrence or distant metastasis. She reported good tolerance to endocrine therapy and maintained a satisfactory quality of life.

Discussion
Breast cancer remains a heterogeneous disease requiring a personalized approach to management. Invasive ductal carcinoma is the most common histological subtype, accounting for approximately 70–80% of cases [3].
Early-stage disease often presents as a painless breast lump, underscoring the importance of breast self-examination and timely clinical evaluation. Imaging modalities such as mammography and ultrasonography play a pivotal role in early detection, while histopathological and molecular characterization guide treatment decisions [4].
This case highlights the significance of multidisciplinary care in optimizing outcomes and emphasizes the favorable prognosis associated with hormone receptor–positive breast cancer when managed appropriately.
Conclusion
Breast cancer should be promptly evaluated in any patient presenting with a suspicious breast lump. Early diagnosis, accurate staging, molecular profiling, and a multidisciplinary treatment approach are essential for achieving optimal clinical outcomes. Continued awareness, screening programs, and individualized therapy remain key components in reducing breast cancer–related morbidity and mortality.
Timely imaging, biopsy, and pathological confirmation allow for risk stratification and treatment planning tailored to tumor biology and patient factors. Ongoing advances in targeted therapies, immunotherapy, and supportive care further contribute to improved survival rates and enhanced quality of life for patients.
References
- Sung H, et al. Global cancer statistics 2020. CA Cancer J Clin. 2021;71(3):209–249.
- Harbeck N, et al. Breast cancer. Nat Rev Dis Primers. 2019;5:66.
- Rakha EA, Ellis IO. Modern classification of breast cancer. Adv Anat Pathol. 2011;18(4):255–267.
- NCCN Clinical Practice Guidelines in Oncology: Breast Cancer. Version 2024.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Sub-Q Ketamine is Safe and Very Effective for Severe Depression.
2.
Study indicates that exercise can help colon cancer survivors live as long as matched individuals
3.
Contradictory Results Are Found in Two Pembrolizumab Trials for Head and Neck Cancer.
4.
Can Concurrent Boost Safely Shorten Breast Cancer Radiation?
5.
Positive Trials; Malignancies Increasing in Younger Adults; Andre Braugher's Cancer Dx.
1.
Trends in Incidence, Care, and Surgery for Medullary Thyroid Cancer: A Review
2.
Antibody-Drug Conjugates in Oncology: Breakthroughs, Clinical Updates, and Pipeline Innovation
3.
Navigating the Stages of Thyroid Cancer: A Guide for Patients
4.
Polycythemia Vera: A Historical Perspective and Contemporary Management
5.
Glofitamab: A Breakthrough Therapy for Relapsed/Refractory Mantle Cell Lymphoma
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Pazopanib: A Game-Changer in Managing Advanced Renal Cell Carcinoma - Part IV
2.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VIII
3.
Evolving Space of First-Line Treatment for Urothelial Carcinoma- Case Discussion
4.
Key Takeaways from The CROWN Trial For ALK + NSCLC Patients with CNS Diseases
5.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part I

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge