Rabies Encephalitis in a Child Following Dog Bite: A Clinicopathological Case Report
OthersPage Navigation
Abstract
Rabies is an acute, progressive, and almost universally fatal viral encephalitis caused by the rabies virus, a member of the Lyssavirus genus. Despite being preventable through timely post-exposure prophylaxis, rabies remains a major public health problem in many low- and middle-income countries, particularly affecting children. The disease is characterized by a prolonged incubation period followed by rapid neurological deterioration once clinical symptoms appear.
We report a fatal case of rabies in a 10-year-old boy following a dog bite, with diagnosis confirmed by the demonstration of Negri bodies in brain tissue. This case underscores the importance of early wound management, timely administration of post-exposure prophylaxis, challenges in clinical diagnosis, and the critical role of preventive strategies, including animal vaccination and public awareness.
Introduction
Rabies is a zoonotic viral disease transmitted primarily through the bite of infected mammals, most commonly dogs. The rabies virus is a neurotropic, single-stranded RNA virus that causes progressive encephalomyelitis once it reaches the central nervous system. Globally, rabies accounts for an estimated 59,000 deaths annually, with children under 15 years constituting a substantial proportion of cases [1].
Although rabies is preventable through prompt post-exposure prophylaxis (PEP), delayed presentation, lack of awareness, and inadequate access to healthcare continue to contribute to rabies-related mortality. Once clinical symptoms manifest, the disease is almost invariably fatal. Classic pathological findings include intracytoplasmic eosinophilic inclusions known as Negri bodies, typically found in neurons of the hippocampus and cerebellum [2].
This case report describes the clinical presentation, diagnostic confirmation, and outcome of rabies in a pediatric patient following a dog bite, highlighting missed opportunities for prevention and the need for strengthened public health measures.
Case Report
Patient History
A 10-year-old boy was brought to the emergency department with complaints of fever, agitation, difficulty swallowing, and episodic involuntary movements for two days. The child had been previously healthy, with no known chronic medical illnesses.
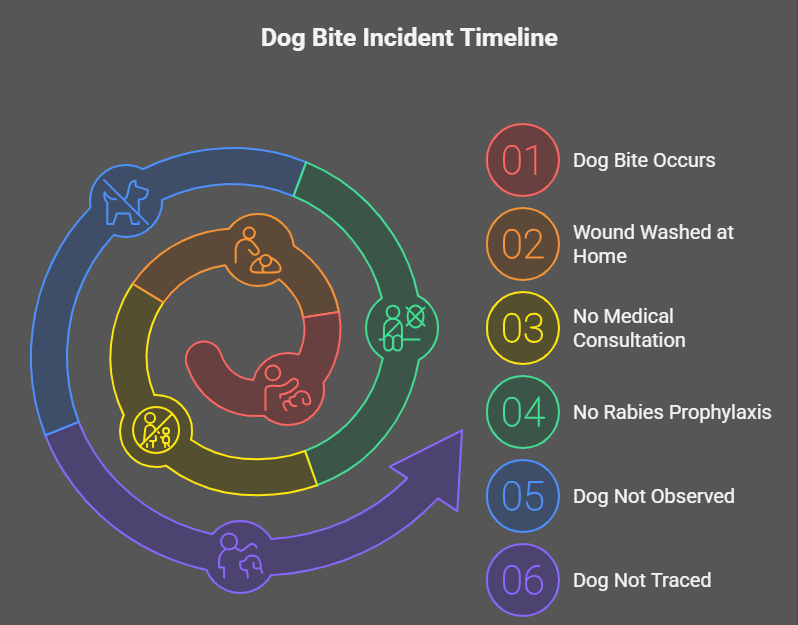
A detailed history revealed that the child had sustained a bite on his right lower leg by a stray dog approximately six weeks prior to presentation. The wound was reportedly superficial and was washed at home with water. No medical consultation was sought at that time, and no rabies post-exposure prophylaxis, including rabies vaccination or rabies immunoglobulin, was administered. The dog was not observed after the incident and could not be traced.
Clinical Examination
On admission, the child appeared acutely ill, anxious, and restless. Vital signs revealed a temperature of 38.8°C, heart rate of 120 beats per minute, blood pressure of 98/60 mmHg, and respiratory rate of 24 breaths per minute. Oxygen saturation was 96% on room air.
Neurological examination showed marked agitation, hypersalivation, and intermittent muscle spasms. Attempts to give oral fluids provoked painful pharyngeal spasms, consistent with hydrophobia. Aerophobia was also noted when air currents triggered distress and spasms. The Glasgow Coma Scale score was 12/15.
Examination of the bite site revealed a healed scar on the right lower leg with no signs of active infection. Cardiovascular, respiratory, and abdominal examinations were otherwise unremarkable.
Clinical Evaluation
Initial Differential Diagnosis
Based on the clinical presentation and history of animal bite, the following differential diagnoses were considered:
• Rabies encephalitis
• Viral meningoencephalitis
• Acute bacterial encephalitis
• Tetanus
• Autoimmune encephalitis
Given the characteristic features of hydrophobia, aerophobia, hypersalivation, and a history of dog bite, rabies was considered the most likely diagnosis.
Investigations
Laboratory Studies
Routine laboratory investigations revealed mild leukocytosis. Serum electrolytes, renal function tests, and liver function tests were within normal limits. Cerebrospinal fluid analysis showed mild lymphocytic pleocytosis with elevated protein levels, findings consistent with viral encephalitis but not specific for rabies.
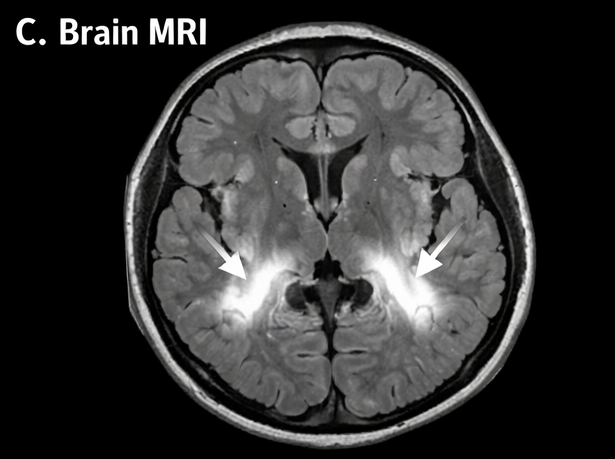
Neuroimaging
Magnetic resonance imaging (MRI) of the brain demonstrated diffuse cerebral edema with hyperintense signals in the brainstem and basal ganglia on T2-weighted and FLAIR sequences, suggestive of encephalitis.
Diagnosis
Despite supportive care, the patient’s neurological status deteriorated rapidly, progressing to coma within 48 hours of admission. The child developed autonomic instability and respiratory failure, necessitating mechanical ventilation.
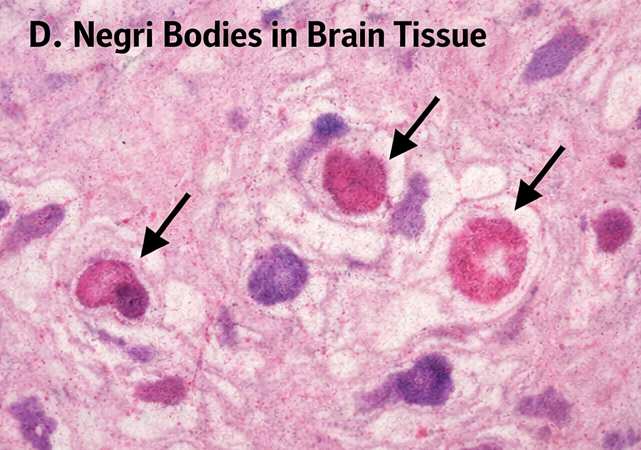
The patient succumbed to the illness on the fifth day of hospitalization. Post-mortem examination of brain tissue was performed. Histopathological analysis revealed the presence of characteristic intracytoplasmic eosinophilic inclusion bodies (Negri bodies) within neurons of the hippocampus and cerebellum, confirming the diagnosis of rabies encephalitis.
The diagnosis was established based on clinical presentation, epidemiological history, and definitive pathological confirmation.
Management and Outcome
Therapeutic Management
Management was primarily supportive, focusing on sedation, control of agitation and seizures, airway protection, and maintenance of hemodynamic stability. The patient was isolated, and barrier nursing precautions were implemented.
No specific antiviral therapy has been proven effective once clinical rabies develops. Rabies post-exposure prophylaxis was not initiated at this stage, as it is ineffective after symptom onset.
Outcome
Despite aggressive supportive management in the intensive care unit, the patient’s condition continued to worsen, culminating in death due to cardiorespiratory failure. The fatal outcome was consistent with the known natural history of symptomatic rabies.
Discussion
Rabies remains one of the deadliest infectious diseases, with near-100% mortality once clinical symptoms appear. Children are particularly vulnerable due to increased exposure to animals and delayed reporting of bites. This case illustrates the classical presentation of rabies, including hydrophobia, aerophobia, and rapid neurological decline.
The long incubation period, typically ranging from weeks to months, offers a critical window for intervention through post-exposure prophylaxis. Immediate wound cleansing, administration of rabies vaccine, and infiltration of rabies immunoglobulin are highly effective in preventing disease if given promptly [3].
Negri bodies, though not always present, remain a hallmark pathological finding and provide definitive evidence of rabies infection. The presence of these inclusions reflects viral replication within neurons and advanced disease progression [4].
This case highlights missed opportunities for prevention and underscores the need for community education regarding dog bite management, improved access to rabies vaccines, and robust animal control programs.
Conclusion
Rabies is a preventable yet fatal disease once clinical manifestations develop. Any dog bite, particularly in children, should be treated as a medical emergency requiring immediate wound care and post-exposure prophylaxis. This case emphasizes the importance of early intervention, public awareness, and coordinated public health strategies to eliminate rabies-related mortality. Strengthening vaccination coverage in both human and animal populations remains essential to achieving rabies elimination goals.
References
- World Health Organization. Rabies fact sheet. WHO; 2023.
- Jackson AC. Rabies: scientific basis of the disease and its management. Lancet. 2013;381(9863):443–452.
- Rupprecht CE, et al. Human rabies prevention—United States, 2008. MMWR Recomm Rep. 2008;57(RR-3):1–28.
- Hemachudha T, et al. Human rabies: neuropathogenesis, diagnosis, and management. Lancet Neurol. 2013;12(5):498–513.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge