Retinal Tear: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Retinal tears are full-thickness breaks in the neurosensory retina that may occur due to vitreoretinal traction, trauma, or degenerative retinal changes. If left untreated, retinal tears can progress to rhegmatogenous retinal detachment, resulting in significant visual impairment or permanent vision loss. Early diagnosis and prompt intervention are essential to preserve vision and prevent complications.
We present the case of a 56-year-old male who presented with sudden onset flashes of light, floaters, and peripheral visual field disturbance in the right eye. Comprehensive ophthalmic examination, dilated fundus evaluation, and retinal imaging confirmed the presence of a superior horseshoe retinal tear associated with posterior vitreous detachment. The patient underwent urgent laser retinopexy, resulting in successful retinal stabilization and preservation of visual acuity.
This case highlights the importance of recognizing warning symptoms of retinal tears and emphasizes the role of early ophthalmologic evaluation and timely treatment in preventing retinal detachment and vision loss.
Introduction
A retinal tear is a full-thickness defect in the retina resulting from vitreoretinal traction. It is a potentially sight-threatening condition because liquefied vitreous can pass through the retinal break and accumulate beneath the retina, leading to retinal detachment.
Retinal tears commonly occur in middle-aged and elderly individuals due to age-related vitreous degeneration and posterior vitreous detachment (PVD). Additional risk factors include high myopia, ocular trauma, previous cataract surgery, retinal degeneration, and family history of retinal detachment.
Several factors increase susceptibility to retinal tears, including:
• Posterior vitreous detachment
• High myopia
• Lattice retinal degeneration
• Ocular trauma
• Previous intraocular surgery
• Family history of retinal detachment
• Increasing age
Important pathological mechanisms include:
• Vitreous liquefaction
• Posterior vitreous separation
• Vitreoretinal traction
• Retinal tissue disruption
• Fluid migration beneath the retina
Common clinical manifestations include:
• Sudden onset floaters
• Photopsia (flashes of light)
• Blurred vision
• Peripheral visual field defects
• Curtain-like shadow in vision
• Visual distortion
Prompt recognition and treatment are critical to prevent progression to retinal detachment.
Case Report
Patient History
A 56-year-old male presented to the ophthalmology emergency department with:
• Sudden onset flashes of light in the right eye for 2 days
• Numerous new floaters
• Mild blurring of vision
• Dark shadow in the superior peripheral visual field
The symptoms began abruptly while reading and progressively increased in intensity.
Past medical and ocular history revealed:
• High myopia since adolescence
• Cataract surgery in the right eye 3 years earlier
• Controlled hypertension
There was no history of:
• Diabetes mellitus
• Ocular infection
• Previous retinal disease
• Recent systemic illness
Clinical Examination
General Examination
• Blood pressure: 132/84 mmHg
• Pulse rate: 78/min
• Temperature: Afebrile
The patient was otherwise clinically stable.
Ophthalmic Examination
Visual Acuity
• Right Eye: 6/9
• Left Eye: 6/6
Intraocular Pressure
• Right Eye: 15 mmHg
• Left Eye: 14 mmHg
Anterior Segment Examination
Slit-lamp examination demonstrated:
• Clear cornea
• Deep anterior chamber
• Well-positioned posterior chamber intraocular lens
• No signs of inflammation
Posterior Segment Examination
Dilated fundus examination of the right eye revealed:
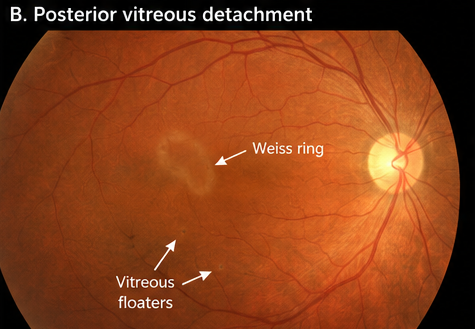
• Posterior vitreous detachment
• Multiple vitreous floaters
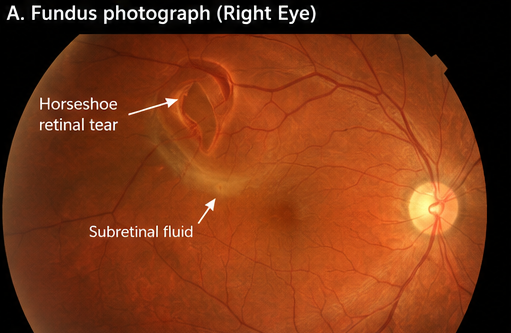
• Superior temporal horseshoe retinal tear measuring approximately 2 disc diameters
• Small surrounding cuff of subretinal fluid
No retinal detachment was identified.
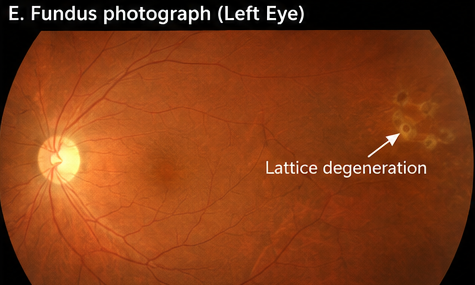
The left eye was normal except for mild peripheral lattice degeneration.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Posterior vitreous detachment without retinal tear
• Retinal tear
• Retinal detachment
• Vitreous hemorrhage
• Ocular migraine
The combination of photopsia, sudden floaters, and funduscopic findings strongly suggested a retinal tear secondary to posterior vitreous detachment.
Investigations
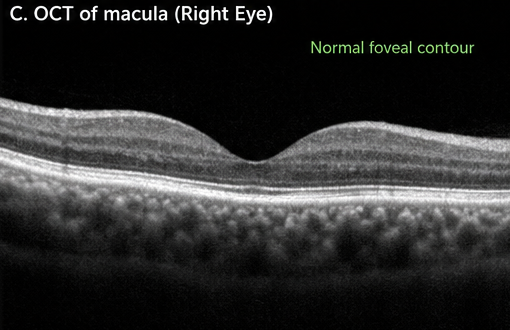
Optical Coherence Tomography (OCT)
Findings included:
• Intact macular architecture
• No macular edema
• No evidence of macular detachment
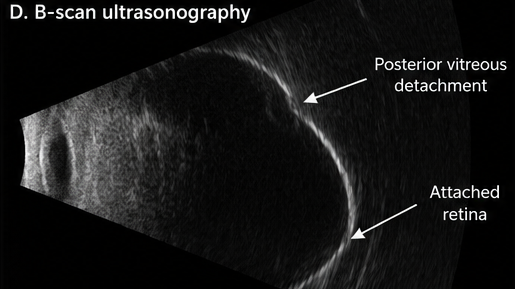
B-Scan Ultrasonography
Performed to assess posterior segment integrity.
Findings included:
• Posterior vitreous detachment
• Mobile vitreous opacities
• Attached retina
Fundus Photography
Demonstrated:
• Horseshoe retinal tear in the superior temporal quadrant
• Localized vitreoretinal traction
• Minimal surrounding subretinal fluid
Diagnosis
Based on clinical examination and retinal imaging findings, a diagnosis of:
Acute Superior Temporal Horseshoe Retinal Tear Associated with Posterior Vitreous Detachment
was established.
Management and Outcome
Initial Management
The patient was advised regarding the risk of progression to retinal detachment and scheduled for urgent intervention.
Management included:
• Patient counseling
• Activity modification
• Detailed retinal examination of both eyes
• Immediate retinal stabilization planning
Laser Retinopexy
Barrier laser photocoagulation was performed around the retinal tear.
The procedure involved:
• Circumferential laser burns surrounding the retinal break
• Creation of a chorioretinal adhesion
• Prevention of subretinal fluid extension
The procedure was completed successfully without complications.
Follow-Up and Clinical Course
At 1 Week
• Reduction in flashes
• Stable vision
• Well-formed laser scars around the tear
• No progression of subretinal fluid
At 1 Month
• Resolution of photopsia
• Significant reduction in floaters
• Stable retinal attachment
At 3 Months
• Visual acuity improved to 6/6
• Retinal tear completely surrounded by mature laser scars
• No evidence of retinal detachment
At 6 Months
• Stable retinal status
• No new retinal tears
• Normal visual function
The patient remained under regular retinal surveillance.
Discussion
Pathophysiology
Retinal tears most commonly develop following posterior vitreous detachment, a natural age-related process in which the vitreous gel separates from the retina.
Key pathological processes include:
• Vitreous liquefaction
• Posterior vitreous collapse
• Vitreoretinal traction
• Retinal break formation
• Subretinal fluid accumulation
Persistent traction may enlarge retinal breaks and increase the risk of retinal detachment.
Epidemiology
Important epidemiological features include:
• Common in individuals over 50 years of age
• More frequent in myopic eyes
• Increased incidence following cataract surgery
• Associated with lattice degeneration
• Significant risk factor for retinal detachment
Approximately 10–15% of symptomatic posterior vitreous detachments may be associated with retinal tears.
Clinical Manifestations
Common symptoms include:
• Flashes of light
• Sudden floaters
• Blurred vision
• Peripheral visual field defects
Characteristic signs include:
• Horseshoe retinal tears
• Operculated retinal holes
• Vitreous hemorrhage
• Posterior vitreous detachment
The sudden appearance of flashes and floaters remains the most important warning sign requiring urgent ophthalmologic evaluation.
Diagnostic Considerations
Diagnosis is primarily based on:
- Detailed patient history
- Dilated retinal examination
- Indirect ophthalmoscopy
- Optical coherence tomography
- Fundus photography
- B-scan ultrasonography
Comprehensive retinal examination remains the gold standard for diagnosis.
Treatment Modalities
Laser Retinopexy
Laser photocoagulation remains the preferred treatment for most retinal tears.
Benefits include:
• Prevention of retinal detachment
• Outpatient procedure
• High success rates
• Minimal recovery time
Cryotherapy
Cryotherapy may be considered when:
• Visualization is difficult
• Tears are located anteriorly
• Laser treatment is not feasible
Surgical Intervention
Vitrectomy or scleral buckle procedures may become necessary if retinal detachment develops.
Complications
Potential complications include:
• Rhegmatogenous retinal detachment
• Vitreous hemorrhage
• Recurrent retinal tears
• Permanent visual loss
• Macular involvement
Early treatment significantly reduces these risks.
Prognosis
The prognosis depends upon:
• Early diagnosis
• Location and size of the tear
• Presence of retinal detachment
• Macular involvement
• Timeliness of treatment
Patients treated before retinal detachment develops generally achieve excellent visual outcomes.
Conclusion
Retinal tears are ophthalmic emergencies that can progress rapidly to retinal detachment and irreversible vision loss if left untreated. Early recognition of warning symptoms such as flashes, floaters, and peripheral visual field defects is essential for timely diagnosis.
This case emphasizes the importance of prompt retinal evaluation, accurate diagnosis, and early laser retinopexy in preventing retinal detachment and preserving visual function. Regular follow-up and patient education remain crucial components of long-term management and visual prognosis.
References
- Byer NE. Natural history of posterior vitreous detachment with early management as the premier line of defense against retinal detachment. https://pubmed.ncbi.nlm.nih.gov/3880367/
- Coffee RE, Westfall AC, Davis GH, Mieler WF, Holz ER. Symptomatic posterior vitreous detachment and the incidence of delayed retinal breaks. https://pubmed.ncbi.nlm.nih.gov/17583667/
- Dayan MR, Jayamanne DG, Andrews RM, Griffiths PG. Flashes and floaters as predictors of vitreoretinal pathology. https://pubmed.ncbi.nlm.nih.gov/9591968/
- American Academy of Ophthalmology. Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration Preferred Practice Pattern®. https://www.aao.org/preferred-practice-pattern/posterior-vitreous-detachment-retinal-breaks-lattice-degeneration-ppp
- American Society of Retina Specialists. Retinal Tears – Patient Information. https://www.asrs.org/patients/retinal-diseases/26/retinal-tears
- National Eye Institute. Retinal Detachment. https://www.nei.nih.gov/learn-about-eye-health/eye-conditions-and-diseases/retinal-detachment
- The Royal College of Ophthalmologists. Retinal Detachment Guidelines. https://www.rcophth.ac.uk
- Mitry D, Charteris DG, Yorston D, Siddiqui MA, Campbell H, Murphy AL, et al. The epidemiology and socioeconomic associations of retinal detachment. https://pubmed.ncbi.nlm.nih.gov/21273233/
- Feltgen N, Walter P. Rhegmatogenous retinal detachment—an ophthalmologic emergency. https://pubmed.ncbi.nlm.nih.gov/21285883/
- World Health Organization. Blindness and Vision Impairment. https://www.who.int/news-room/fact-sheets/detail/blindness-and-vision-impairment
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Chris Hoy reveals that he has terminal cancer?here's how to spot early signs of prostate cancer
2.
Check for eating disorders in bipolar disorder patients.
3.
Rising rates of head and neck cancers in England
4.
Q&A: Why adolescents and young adults with cancer are falling behind
5.
Including Bereavement in the Care Continuum.
1.
Thyroidectomy & Survival: Highlights from ASCO 2025 and Current U.S. Findings
2.
Uncovering the Mysteries of the RDW Blood Test
3.
Breakthroughs in Cancer Care: From Rare Diagnoses to Advanced and Early-Stage Treatments
4.
AI in Cancer Diagnostics and Imaging Interpretation
5.
Subchorionic Hematoma: Causes, Symptoms, and Treatment
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
2.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI
3.
Current Scenario of Cancer- Q&A Session to Close the Gap Part II
4.
Understanding the Evolution in Lung Cancer- An Initiative from Manipal Hospitals: Further Discussion
5.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge