Bullet Injury to the Chest: Clinical Presentation, Diagnostic Challenges, Management, and Outcomes - A Case Report
OthersPage Navigation
Abstract
Penetrating chest trauma due to firearm-related injury is a potentially life-threatening emergency associated with high morbidity and mortality, depending on the trajectory of the projectile and the structures involved. Such injuries may affect the lungs, heart, great vessels, and mediastinal organs, often presenting with variable clinical severity. We report a confirmed case of a retained bullet injury to the chest in a young adult male presenting with chest pain and dyspnea following a firearm assault. This case highlights the clinical presentation, diagnostic challenges, imaging evaluation, multidisciplinary management approach, surgical considerations, and clinical outcome. The report emphasizes the importance of early trauma assessment, rapid imaging, hemodynamic stabilization, timely surgical intervention when indicated, and structured follow-up to prevent delayed complications such as infection, hemothorax, pneumothorax, and vascular injury.
Introduction
Firearm-related chest injuries represent a significant subset of penetrating thoracic trauma and are associated with high rates of organ injury, hemorrhage, and mortality. The thorax houses vital structures including the lungs, heart, great vessels, esophagus, and tracheobronchial tree, making penetrating trauma in this region particularly dangerous. The severity of injury depends on projectile velocity, trajectory, distance from the source, and secondary fragmentation. Clinical presentation ranges from minimal symptoms to hemorrhagic shock and respiratory failure. Prompt recognition, adherence to Advanced Trauma Life Support (ATLS) principles, rapid imaging, and early surgical consultation are essential to optimize outcomes. This case report describes the presentation, diagnostic workup, management strategy, and outcome of a patient with a retained bullet in the chest following firearm injury.
Case Report
Patient History
A 27-year-old man was brought to the emergency department following a firearm assault with a single gunshot wound to the left anterior chest. The incident had occurred approximately 45 minutes prior to presentation. The patient complained of acute left-sided chest pain and shortness of breath. There was no loss of consciousness. He had no prior history of cardiopulmonary disease or bleeding disorders. He was not on anticoagulant therapy and had no known comorbidities. There was no history of substance abuse.
Clinical Examination
On arrival, the patient was conscious and oriented. Vital signs revealed tachycardia (heart rate 118/min), blood pressure 98/60 mmHg, respiratory rate 26/min, and oxygen saturation 90% on room air. Examination showed a single entry wound over the left anterior chest in the fifth intercostal space, with no obvious exit wound.
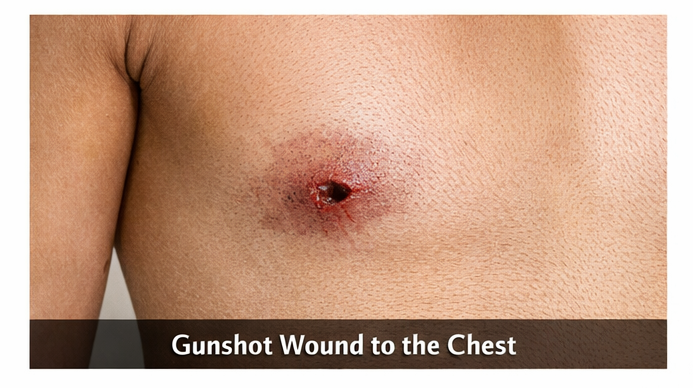
Breath sounds were reduced on the left side. There was mild subcutaneous emphysema over the left chest wall. The trachea was midline. No signs of pericardial tamponade or external hemorrhage were noted. The abdomen and neurological examination were unremarkable.
Clinical Evaluation
Differential Diagnosis
The differential diagnoses included:
• Penetrating lung injury with pneumothorax
• Hemothorax
• Pulmonary contusion
• Cardiac or pericardial injury
• Great vessel injury
• Retained intrathoracic foreign body (bullet)
Investigations
Initial bedside ultrasonography (eFAST) revealed a left-sided pneumothorax with a small hemothorax and no pericardial effusion.
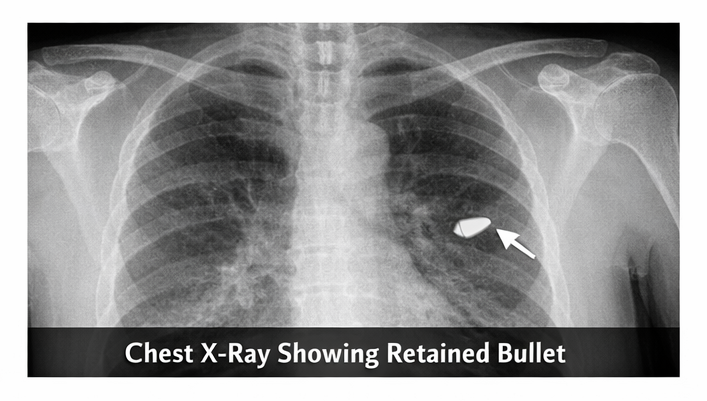
Chest radiography demonstrated a radio-opaque foreign body consistent with a retained bullet in the left hemithorax with partial lung collapse.
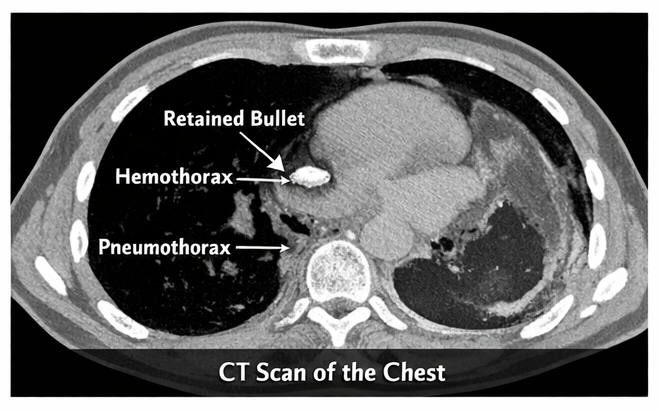
Contrast-enhanced computed tomography (CT) of the chest confirmed a retained bullet lodged in the posterior segment of the left lower lobe, associated with pulmonary laceration, moderate hemothorax, and pneumothorax. No major vascular or cardiac injury was identified. Baseline laboratory investigations showed mild anemia and elevated inflammatory markers.
Diagnosis
Based on clinical findings and imaging, a diagnosis of penetrating chest trauma due to firearm injury with retained intrapulmonary bullet, associated pneumothorax and hemothorax, was established.
Management and Outcome
Management Strategy
The patient was managed according to ATLS principles. Initial stabilization included oxygen supplementation, intravenous fluid resuscitation, and analgesia. A left-sided intercostal chest tube was inserted, draining approximately 600 mL of blood and air, with subsequent improvement in respiratory distress and oxygen saturation.
Broad-spectrum intravenous antibiotics and tetanus prophylaxis were administered.
Cardiothoracic surgical consultation was obtained. Given the patient’s hemodynamic stability, absence of major vascular or cardiac injury, and controlled hemothorax with chest tube drainage, conservative management with close monitoring was initially chosen. The retained bullet was not removed emergently due to its deep intrapulmonary location and lack of immediate complications. The patient was closely observed for signs of ongoing bleeding, infection, air leak, or respiratory compromise.
Follow-Up and Outcome
Over the next 72 hours, the patient remained hemodynamically stable with decreasing chest tube output and improving lung expansion on serial chest radiographs. The chest tube was removed on day 5 following radiographic confirmation of lung re-expansion and resolution of air leak. The patient was discharged on day 7 with oral antibiotics and analgesics.
At 1-month follow-up, the patient was asymptomatic, with normal respiratory examination and no radiological evidence of residual pneumothorax or hemothorax. The retained bullet remained in situ without complications. Surgical removal was deferred, and the patient was counseled regarding warning symptoms such as fever, hemoptysis, or worsening chest pain. At 6-month follow-up, no late complications were noted.
Discussion
Penetrating chest trauma due to firearm injury poses significant diagnostic and therapeutic challenges. The clinical severity depends on the structures involved and the energy transferred by the projectile. Lung injury is the most common consequence, often resulting in pneumothorax, hemothorax, or pulmonary contusion. eFAST and chest radiography are essential initial diagnostic tools, while contrast-enhanced CT provides detailed assessment of intrathoracic injury and projectile trajectory.
Management follows ATLS protocols, prioritizing airway, breathing, and circulation. Chest tube thoracostomy remains the cornerstone of treatment for pneumothorax and hemothorax. Surgical intervention is indicated in cases of massive hemothorax, ongoing bleeding, cardiac injury, major vascular injury, or retained foreign bodies causing infection or functional compromise. Retained bullets may be left in situ if asymptomatic and not associated with contamination, vascular injury, or risk of migration. Long-term follow-up is important to monitor for delayed complications such as infection, fibrosis, bronchopleural fistula, or hemoptysis.
Conclusion
Firearm-related penetrating chest injuries constitute a medical emergency requiring rapid assessment, multidisciplinary coordination, and timely intervention. This case highlights the importance of structured trauma evaluation, early imaging, and individualized management strategies based on hemodynamic status and injury pattern. Conservative management of a retained intrapulmonary bullet can be successful in selected stable patients without major vascular or cardiac involvement. Comprehensive follow-up is essential to detect late complications and ensure optimal functional recovery. Early trauma care, appropriate imaging, chest tube management, judicious surgical decision-making, and close surveillance collectively contribute to favorable clinical outcomes in penetrating thoracic injuries.
References
- Demetriades D, Murray J, Charalambides K, et al. Trauma fatalities: Time and location of hospital deaths. J Am Coll Surg. 2004;198(1):20–26.
- Advanced Trauma Life Support (ATLS®): Student Course Manual. 10th ed. American College of Surgeons; 2018.
- Karmy-Jones R, Jurkovich GJ, Shatz DV, et al. Management of traumatic lung injury. Surg Clin North Am. 2001;81(6):1407–1425.
- Demetriades D, Velmahos GC. Penetrating injuries of the chest: Indications for operation. Scand J Surg. 2002;91(1):41–45.
- Shorr RM, Crittenden M, Indeck M, et al. Blunt thoracic trauma: Analysis of 515 patients. Ann Surg. 1987;206(2):200–205.
- Navsaria PH, Nicol AJ, Ball CG. Penetrating thoracic trauma. In: Trauma, 9th ed. McGraw-Hill; 2020.
- Karmy-Jones R, Namias N, Coimbra R, et al. Western Trauma Association critical decisions in trauma: Penetrating chest trauma. J Trauma Acute Care Surg. 2014;77(6):994–1002.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Charles III, King of Kings, is Cancerous.
2.
Chemo-Free Quadruplet Shows Promise as DLBCL's First Therapy.
3.
Perioperative Anti-PD-1 in Soft-Tissue Sarcoma Boosts Disease-Free Survival
4.
Merck enhances its oncology pipeline by means of a strategic alliance with Hengrui.
5.
WHO releases new R&D landscape analyses highlighting gaps and inequities in cancer research
1.
The benefits and risks of taking fludrocortisone for adrenal insufficiency
2.
Ultimate Guide to Oncology Services in the USA
3.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
4.
Real-World Oncology Insights: CAR-T, Immunotherapy, PROs, and Digital Tools
5.
Introducing the Corrected Calcium Calculator: A Revolutionary Tool in Medical Assessment
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Oropharyngeal Cancer in Relation to HPV Status
2.
Advances in Classification/ Risk Stratification of Plasma Cell Dyscrasias- The Summary
3.
Navigating the Brain Barrier: The CNS Challenge in ALK+ NSCLC
4.
EGFR Mutation Positive Non-Small Cell Lung Cancer- Case Discussion & Conclusion
5.
Management of 1st line ALK+ mNSCLC (CROWN TRIAL Update) - Part V

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge