Goitre: Clinical Evaluation, Multidisciplinary Management, and Outcome - A Case Report
OthersPage Navigation
Abstract
Goitre, defined as an abnormal enlargement of the thyroid gland, is a common endocrine disorder encountered worldwide, particularly in regions with iodine deficiency. The condition may arise from a wide spectrum of etiologies, including iodine deficiency, autoimmune thyroid disease, multinodular hyperplasia, and thyroid neoplasms. Clinical presentation varies from an asymptomatic neck swelling to significant compressive symptoms and thyroid dysfunction. Accurate diagnosis requires a comprehensive assessment encompassing clinical evaluation, biochemical testing, imaging, and cytological analysis to determine functional status and malignancy risk. Management strategies range from observation and medical therapy to definitive surgical intervention. We report a case of a euthyroid multinodular goitre in a middle-aged female presenting with progressive neck swelling and compressive symptoms. A structured multidisciplinary approach involving endocrinology, radiology, and endocrine surgery resulted in successful surgical management with excellent functional and cosmetic outcomes. This case highlights the importance of timely diagnosis, individualized treatment planning, and coordinated care in optimizing outcomes for patients with goitre.
Introduction
Goitre remains one of the most prevalent thyroid disorders globally and continues to pose a significant public health burden, particularly in developing countries and regions with inadequate iodine intake [1]. The term “goitre” encompasses a broad range of thyroid enlargements that may be diffuse or nodular and may be associated with euthyroid, hypothyroid, or hyperthyroid states.
The pathogenesis of goitre is multifactorial. Chronic iodine deficiency leads to reduced thyroid hormone synthesis, resulting in sustained thyroid-stimulating hormone (TSH) stimulation and compensatory glandular hypertrophy and hyperplasia. Other causes include autoimmune thyroid diseases such as Graves’ disease and Hashimoto’s thyroiditis, genetic defects in thyroid hormone synthesis, multinodular hyperplasia, and thyroid malignancies [2].
Although many goitres are benign and asymptomatic, progressive enlargement can result in compressive symptoms involving the trachea, esophagus, and recurrent laryngeal nerve. In addition, the presence of thyroid nodules necessitates careful evaluation to exclude malignancy. Advances in imaging, cytology, and surgical techniques have significantly improved diagnostic accuracy and treatment outcomes.
This case report describes the clinical presentation, diagnostic evaluation, and management of a multinodular goitre, emphasizing the role of a multidisciplinary approach in achieving favorable patient outcomes.
Case Report
Patient History
A 48-year-old female presented to the endocrine surgery outpatient clinic with a gradually enlarging anterior neck swelling for approximately four years. The swelling had increased slowly in size and was initially asymptomatic.

Over the preceding six months, the patient experienced a sensation of neck tightness and intermittent dysphagia, particularly for solid foods. There was no history of dyspnea, orthopnea, stridor, or change in voice.
The patient denied symptoms suggestive of thyroid hormone excess or deficiency, including weight changes, heat or cold intolerance, palpitations, tremors, constipation, or fatigue. There was no history of neck irradiation, prior thyroid surgery, or known thyroid disease. Family history was negative for thyroid malignancy or autoimmune thyroid disorders.
She had no significant comorbidities and was not on long-term medications. The patient resided in a semi-urban area with historically borderline iodine intake.
Clinical Examination
On general examination, the patient was alert, comfortable, and clinically euthyroid. Vital signs were within normal limits. There were no signs of thyrotoxicosis or hypothyroidism.
Local examination of the neck revealed a visibly enlarged thyroid gland occupying the anterior neck region. Palpation demonstrated a multinodular thyroid enlargement involving both lobes, with the right lobe more prominently affected. The swelling moved with deglutition, was firm in consistency, non-tender, and had an irregular nodular surface. The lower border of the gland was palpable, suggesting no retrosternal extension.
There was no cervical lymphadenopathy. Pemberton’s sign was negative, indicating the absence of significant thoracic inlet obstruction. Indirect laryngoscopy revealed normal vocal cord mobility bilaterally.
Investigations
Laboratory Studies
Thyroid function tests demonstrated normal serum TSH, free thyroxine (FT4), and triiodothyronine (T3) levels, confirming a euthyroid state. Thyroid peroxidase and thyroglobulin antibodies were negative, reducing the likelihood of autoimmune thyroiditis. Routine hematological and biochemical investigations were within normal limits.
Imaging Studies
High-resolution ultrasonography of the neck revealed an enlarged thyroid gland with multiple nodules of varying sizes and echotexture in both lobes.

The dominant nodule in the right lobe measured 3.5 × 2.8 cm and demonstrated mixed echogenicity without microcalcifications, irregular margins, or increased intranodular vascularity.
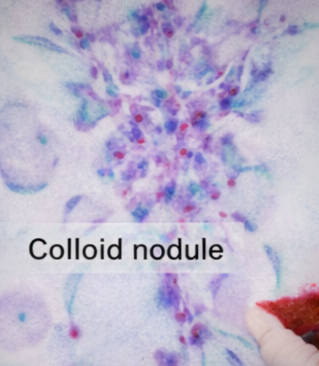
Fine-needle aspiration cytology (FNAC) of the dominant nodule was performed under ultrasound guidance and reported as benign colloid nodule, corresponding to Bethesda category II.
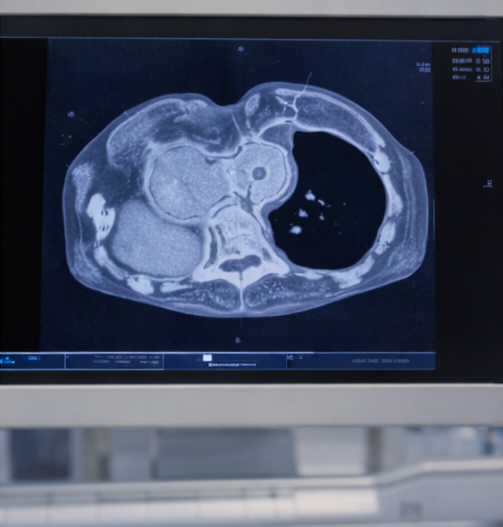
A contrast-enhanced computed tomography (CT) scan of the neck was obtained to assess tracheal compression and retrosternal extension. The imaging showed mild tracheal deviation without significant narrowing and no substernal extension.
Diagnosis
Based on clinical presentation, imaging findings, and cytological analysis, a diagnosis of euthyroid multinodular goitre with compressive symptoms was established.
Management and Outcome
Multidisciplinary Approach
The patient was managed through a coordinated multidisciplinary team comprising endocrinologists, endocrine surgeons, radiologists, anesthesiologists, and nursing staff. Given the progressive enlargement, presence of compressive symptoms, and bilateral nodular involvement, surgical intervention was recommended.
Preoperative counseling included discussion of surgical options, potential risks such as recurrent laryngeal nerve injury and hypocalcemia, and the need for lifelong thyroid hormone replacement therapy following total thyroidectomy.
Surgical Management
The patient underwent an elective total thyroidectomy under general anesthesia. Intraoperatively, the thyroid gland was markedly enlarged and multinodular but well-encapsulated. Both recurrent laryngeal nerves were carefully identified and preserved. The parathyroid glands were visualized and protected, with adequate vascular supply maintained.
Hemostasis was meticulously achieved, and a closed suction drain was placed. The procedure was completed without intraoperative complications.
Histopathological Findings
Gross examination of the surgical specimen revealed an enlarged multinodular thyroid gland. Histopathological analysis confirmed the diagnosis of multinodular colloid goitre, characterized by variably sized follicles filled with colloid and areas of nodular hyperplasia. There was no evidence of malignancy.
Postoperative Course and Follow-Up
The postoperative period was uneventful. Serum calcium levels remained within normal limits, and there were no signs of hypocalcemia. Vocal cord function was assessed postoperatively and found to be intact.
The patient was initiated on levothyroxine replacement therapy and discharged on postoperative day three. At six-week and three-month follow-up visits, she reported complete resolution of compressive symptoms and significant improvement in quality of life. Thyroid hormone levels were well controlled, and the surgical scar healed satisfactorily with good cosmetic outcome.
Discussion
Multinodular goitre represents a common endpoint of chronic thyroid stimulation, often related to iodine deficiency and genetic susceptibility [3]. While many goitres remain asymptomatic, progressive enlargement can lead to compressive symptoms and cosmetic concerns, necessitating intervention.
Accurate assessment of thyroid nodules is critical to exclude malignancy. High-resolution ultrasound and FNAC remain the cornerstone of evaluation, with CT imaging playing an important role in assessing retrosternal extension and airway compromise [4].
Surgical management is indicated in patients with symptomatic goitres, suspicion of malignancy, retrosternal extension, or significant cosmetic deformity. Total thyroidectomy is increasingly favored in multinodular disease due to lower recurrence rates and definitive treatment, albeit with the requirement for lifelong hormone replacement [5].
This case underscores the importance of a structured diagnostic approach and multidisciplinary collaboration in achieving optimal surgical and functional outcomes.
Conclusion
Goitre is a common endocrine disorder with diverse etiologies and clinical manifestations. Comprehensive clinical evaluation, biochemical testing, imaging, and cytological assessment are essential to determine the underlying cause and guide management. This case demonstrates that timely surgical intervention for symptomatic multinodular goitre, supported by coordinated multidisciplinary care, results in excellent clinical outcomes, symptom resolution, and improved quality of life. Early diagnosis, patient education, and long-term follow-up remain critical in preventing complications and recurrence.
References
-
Zimmermann MB. Iodine deficiency. Endocr Rev. 2009;30(4):376–408.
-
Vanderpump MPJ. The epidemiology of thyroid disease. Br Med Bull. 2011;99:39–51.
-
Brent GA. Clinical practice: Graves’ disease. N Engl J Med. 2008;358(24):2594–2605.
-
Haugen BR, et al. 2015 American Thyroid Association management guidelines. Thyroid. 2016;26(1):1–133.
-
De Groot LJ, et al. Management of benign multinodular goitre. Endocr Rev. 2012;33(5):593–646.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Year in Review: Chronic Lymphocytic Leukemia
2.
According to a study, white Americans are overdiagnosing melanoma at an alarming rate.
3.
Approval in Endometrial Cancer Expanded; Masks at Cancer Centers; NPR Reporter Dies
4.
The First Gene Therapy Provides a Durable Response for Non-Muscle-Invasive Bladder Cancer.
5.
Canine Cancer Vaccine: A Potential Resurrection? U.S. KK. Snubs Enertu.
1.
What Is Carboxyhemoglobin And How Can It Affect Your Health?
2.
Lu-177 Vipivotide in Prostate Cancer: A Breakthrough in Radioligand Therapy
3.
Unraveling the Mysteries of Coagulopathy: A Comprehensive Definition
4.
Machine Learning in Genomic Analysis for Early Lung Cancer Detection: Key Advances and Insights
5.
A New Perspective on Spherocytosis: Uncovering Innovative Treatments
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Revolutionizing Treatment of ALK Rearranged NSCLC with Lorlatinib - Part II
2.
Navigating the Complexities of Ph Negative ALL - Part XIII
3.
Updates on the First Line Management of ALK+ NSCLC
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
Breaking Ground: ALK-Positive Lung Cancer Front-Line Management - Part II

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge