Ludwig’s Angina in a Pediatric Patient Following Untreated Dental Infection: A Case Report
OthersPage Navigation
Abstract
Ludwig’s angina is a rapidly progressive, potentially life-threatening cellulitis involving the floor of the mouth and submandibular spaces, most commonly arising from odontogenic infections. Although more frequently reported in adults, pediatric cases pose significant diagnostic and airway management challenges due to rapid disease progression and smaller airway caliber. We report a case of a 6-year-old child presenting with acute onset of painful swelling of the floor of the mouth and submandibular region, associated with drooling, dysphagia, fever, and respiratory distress following an untreated dental infection. Prompt clinical recognition, airway assessment, and aggressive medical management resulted in a favorable outcome. This case underscores the importance of early diagnosis and timely intervention in preventing life-threatening complications of Ludwig’s angina in children.
Introduction
Ludwig’s angina is an aggressive, diffuse cellulitis of the submandibular, sublingual, and submental spaces that can rapidly compromise the airway if not promptly treated [1,2]. The condition is most commonly of odontogenic origin, particularly involving infections of the mandibular molars, which allow direct spread into the deep neck spaces [3]. Clinical features typically include firm swelling of the floor of the mouth, elevation of the tongue, dysphagia, drooling, fever, and varying degrees of respiratory distress.
In pediatric patients, Ludwig’s angina is relatively uncommon but carries a higher risk of rapid deterioration due to anatomical and physiological factors, including narrower airways and limited physiological reserve [4]. Early recognition and prompt multidisciplinary management are critical to reduce morbidity and mortality. We present a case of Ludwig’s angina in a 6-year-old child following an untreated dental infection, highlighting key clinical features, diagnostic considerations, and management principles.
Case Report
Patient History
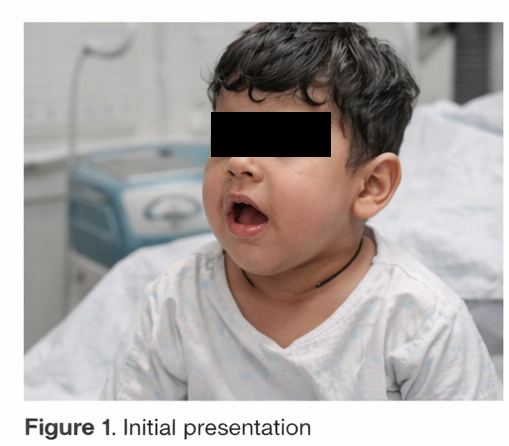
A 6-year-old child was brought to the emergency department with a 2-day history of rapidly progressive swelling of the floor of the mouth and submandibular region. The swelling was associated with significant pain, fever, drooling, difficulty swallowing, and progressive breathing difficulty. The caregivers reported a preceding history of toothache involving the lower molar region approximately one week prior, for which no dental or medical treatment had been sought.
The child had increasing discomfort while eating and speaking, and preferred to sit upright due to worsening respiratory symptoms. There was no history of trauma, foreign body ingestion, or prior similar episodes. The child had no known chronic medical conditions, immunodeficiency, or previous hospitalizations.
Clinical Findings
On examination, the child appeared ill, febrile, and anxious, with signs of respiratory distress. Vital signs revealed tachycardia, fever, and mildly increased respiratory rate. Inspection of the oral cavity demonstrated marked swelling and induration of the floor of the mouth with elevation and posterior displacement of the tongue. Mouth opening was limited due to pain and edema, and drooling was evident.
External examination revealed firm, tender, bilateral submandibular swelling with overlying skin appearing tense but without erythema or fluctuance.
Palpation confirmed a “woody” induration of the submandibular region. Cervical lymphadenopathy was present. No obvious abscess or purulent discharge was noted intraorally. These findings raised strong clinical suspicion for Ludwig’s angina with impending airway compromise.
Investigations
Laboratory investigations revealed marked leukocytosis with a neutrophilic predominance, along with elevated inflammatory markers, indicating an acute bacterial inflammatory process. Blood cultures were obtained prior to the initiation of antimicrobial therapy to help identify the causative organism and guide targeted treatment if necessary. Additional baseline biochemical parameters were monitored to assess the patient’s overall clinical status and to establish reference values during treatment.
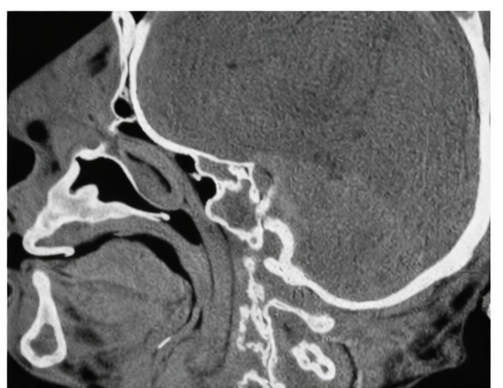
Contrast-enhanced computed tomography of the neck demonstrated diffuse inflammatory involvement of the submandibular and sublingual spaces, characterized by soft tissue edema and prominent fat stranding, without evidence of a well-defined or drainable abscess collection. Imaging also showed elevation and posterior displacement of the tongue with resultant narrowing of the upper airway due to surrounding soft tissue swelling. These radiological findings, in conjunction with the clinical presentation, were consistent with the diagnosis of Ludwig’s angina and highlighted the significant risk of airway compromise, underscoring the need for urgent and aggressive management.
Management and Outcome
The patient was immediately admitted to a high-dependency unit for close airway monitoring. A multidisciplinary team involving pediatrics, otolaryngology, anesthesiology, and dentistry was engaged early. Broad-spectrum intravenous antibiotics covering aerobic and anaerobic organisms were initiated promptly. Supportive care included intravenous fluids, antipyretics, and oxygen supplementation.
Given the risk of airway compromise, the child was closely observed for any signs of deterioration. Dental evaluation identified an infected mandibular molar as the likely source, which was managed once the acute infection was controlled.

Surgical drainage was not required, as no discrete abscess was identified and the patient demonstrated clinical improvement with medical therapy alone.
Over the next several days, the swelling gradually subsided, respiratory symptoms resolved, and the child was able to tolerate oral intake. The patient was transitioned to oral antibiotics and discharged with close outpatient follow-up.

At follow-up, complete resolution of symptoms was noted, with no residual complications.

Discussion
Ludwig’s angina is a medical and surgical emergency characterized by rapidly spreading cellulitis of the submandibular spaces, with the potential for sudden airway obstruction [1,3]. Odontogenic infections remain the most common precipitating factor, particularly untreated infections of the lower molars. In children, early symptoms may be subtle but can progress rapidly, emphasizing the need for heightened clinical vigilance.
The hallmark clinical features include painful submandibular swelling, induration of the floor of the mouth, tongue elevation, dysphagia, drooling, and respiratory distress. Imaging, particularly contrast-enhanced CT, is useful in assessing disease extent and identifying abscess formation, although treatment should not be delayed in unstable patients [4,5].
Airway management remains the cornerstone of treatment, followed by prompt initiation of broad-spectrum antibiotics targeting polymicrobial oral flora. Surgical intervention is reserved for cases with abscess formation or failure of medical therapy. With early recognition and appropriate multidisciplinary management, outcomes are generally favorable, even in pediatric patients.
Conclusion
Ludwig’s angina should be strongly considered in pediatric patients who present with rapidly progressive swelling of the submandibular region and floor of the mouth, particularly when there is a preceding history of untreated or inadequately treated dental infections. The presence of associated symptoms such as drooling, dysphagia, fever, trismus, tongue elevation, and respiratory distress should heighten clinical suspicion, as these features may indicate evolving airway compromise and rapid disease progression.
Early recognition of these characteristic clinical signs, combined with prompt and thorough airway assessment, is critical to preventing life-threatening complications such as acute airway obstruction, sepsis, and mediastinal spread of infection. Immediate initiation of broad-spectrum intravenous antibiotics targeting aerobic and anaerobic oral flora remains the cornerstone of management, alongside close monitoring in an appropriate care setting. Increased awareness among clinicians, dentists, and caregivers regarding the potential severity and rapid progression of odontogenic infections in children is essential to facilitate early referral, timely intervention, and improved clinical outcomes.
References
- Grover S, et al. Ludwig’s angina: A review of current airway management. Int J Crit Illn Inj Sci. 2015;5(2):96–100.
- Britt JC, et al. Ludwig’s angina in the pediatric population: Report of a case and review of the literature. Int J Pediatr Otorhinolaryngol. 2000;52(1):79–87.
- Moreland LW, Corey J, McKenzie R. Ludwig’s angina: Report of a case and review of the literature. Arch Intern Med. 1988;148(2):461–466.
- Brook I. Microbiology and management of deep facial infections and Ludwig’s angina. J Oral Maxillofac Surg. 2003;61(4):455–460.
- Huang TT, et al. Deep neck infection: Analysis of 185 cases. Head Neck. 2004;26(10):854–860.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
PET-CT finds further-reaching metastases in patients with locally advanced breast cancer.
2.
Reasons Behind Refusing Stem Cell Transplantation in Certain Myeloma Patients.
3.
Hospitalization and mortality rates are associated with exposure to the omicron variant of COVID-19 in patients with solid cancer.
4.
AI System Beats Radiologists in Detecting Clinically Significant Prostate Cancer
5.
In heavily pretreated DLBCL, Triplet Scores a Survival Victory.
1.
The Precision Revolution: Bispecific Antibodies and Antibody-Drug Conjugates Reshaping the Oncology Landscape
2.
Is AI The New Radiologist For Breast MRI?
3.
Uncovering New Hope for Follicular Lymphoma Patients
4.
The Silent Signs: Uncovering Stomach Cancer Symptoms Before It's Too Late
5.
Unveiling the Chadwick Sign: A Revolutionary New Tool for Detecting Early Signs of Cancer
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
CDK4/6 Inhibitors Redefining Treatment for HR+/HER2- aBC In Post-Menopausal Women- A Panel Discussion
2.
Efficient Management of First line ALK-rearranged NSCLC - Part V
3.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
4.
Updates on Standard V/S High Risk Myeloma Treatment- The Next Part
5.
Current Cancer Scenario in India- Importance of Genomic Testing & Advancement in Diagnosis and Treatment

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge