Dermoid Cyst of the Eye: Clinical Evaluation, Multidisciplinary Management, and Outcome - A Case Report
OthersPage Navigation
Abstract
Dermoid cysts are benign, congenital developmental lesions resulting from ectodermal tissue entrapment along embryonic fusion lines. In ophthalmic practice, dermoid cysts represent one of the most common non-inflammatory orbital and periocular masses in pediatric patients. These lesions are typically slow growing, painless, and present early in life, most often in the superotemporal orbital region. Although benign, dermoid cysts may pose diagnostic challenges due to their variable depth, potential for intraorbital extension, and similarity to other congenital or acquired periocular masses.
We present a case of a periocular dermoid cyst in a pediatric patient presenting with a gradually enlarging, asymptomatic swelling near the lateral canthus. This case emphasizes the importance of comprehensive clinical evaluation, appropriate imaging to assess lesion extent, histopathological confirmation, and a multidisciplinary management approach to ensure complete excision, minimize complications, and achieve optimal functional and cosmetic outcomes.
Introduction
Dermoid cysts are congenital choristomas that arise from sequestration of surface ectoderm along embryonic suture lines during fetal development. These cysts are lined by stratified squamous epithelium and contain dermal appendages such as hair follicles, sebaceous glands, and sweat glands. In the orbital and periocular region, dermoid cysts account for a significant proportion of pediatric orbital tumors and are among the most frequently encountered congenital lesions by ophthalmologists and pediatric surgeons [1].
Ocular dermoid cysts commonly occur near the frontozygomatic suture at the superotemporal aspect of the orbit, though they may also be found medially, intraorbitally, or rarely with intracranial extension. While most lesions are superficial and easily diagnosed clinically, deeper dermoid cysts may present later in childhood or adolescence with proptosis, globe displacement, or restricted ocular motility [2].
Early identification and appropriate management are essential to prevent complications such as rupture, inflammation, infection, bony erosion, or cosmetic deformity. Differentiation from other periocular lesions—including epidermoid cysts, hemangiomas, lymphangiomas, lacrimal gland tumors, and malignant orbital masses—is critical for appropriate treatment planning. Imaging plays a pivotal role in determining lesion extent and surgical approach.
Case Report
Patient History
A 7-year-old male child was presented to the ophthalmology outpatient department with a complaint of a swelling near the outer corner of the right eye. According to the parents, the swelling had been noticed since early childhood but had become more prominent over the past year. The increase in size was gradual and not associated with pain, redness, discharge, or visual disturbance.

There was no history of trauma, fever, weight loss, headache, or neurological symptoms. The child did not experience diplopia, watering, or difficulty in eye movements. There was no history of similar lesions in the family. The patient had achieved normal developmental milestones and had no significant past medical or surgical history.
Clinical Examination
On general examination, the child was alert, cooperative, and systemically stable. Vital signs were within normal limits, and there were no features suggestive of syndromic associations or systemic illness.
Ocular examination revealed best-corrected visual acuity appropriate for age in both eyes. External examination showed a well-defined, firm, non-tender, non-compressible mass measuring approximately 2 × 2 cm located at the superotemporal aspect of the right orbit near the lateral eyebrow. The lesion was immobile and appeared fixed to the underlying structures, consistent with a lesion arising along an orbital suture line. The overlying skin was normal in color and texture, with no evidence of inflammation or sinus formation.

There was no pulsation or change in size with Valsalva maneuver. Extraocular movements were full in all directions, with no restriction or pain. Pupillary reactions were normal, and there was no afferent pupillary defect. Slit-lamp examination of the anterior segment and fundus examination of both eyes were unremarkable. Intraocular pressure was within normal limits.
Clinical Evaluation
Differential Diagnosis
Based on the congenital onset, slow progression, firm consistency, and characteristic location, the following differential diagnoses were considered:
• Dermoid cyst
• Epidermoid cyst
• Lacrimal gland mass
• Capillary hemangioma
• Lymphangioma
• Pilomatrixoma
Given the absence of vascular signs, inflammatory features, or rapid growth, a benign congenital lesion was strongly suspected, with dermoid cyst being the most likely diagnosis.
Investigations
Radiological Evaluation
To assess the depth, extent, and relationship of the lesion to adjacent orbital structures, imaging was performed.
A computed tomography (CT) scan of the orbits revealed a well-circumscribed, hypodense lesion located in the superotemporal extraconal space of the right orbit. The lesion demonstrated fat attenuation and caused mild pressure remodeling of the adjacent frontal bone without cortical breach or erosion. There was no enhancement after contrast administration and no evidence of intracranial extension.
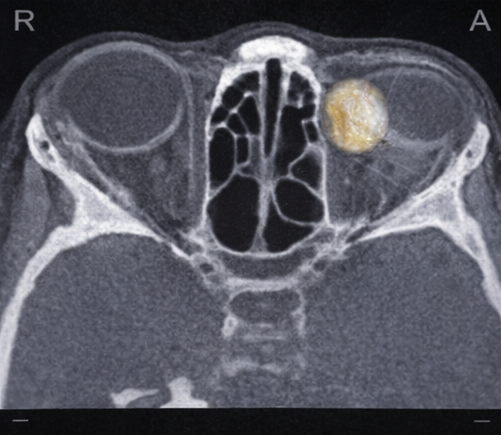
These imaging features were highly suggestive of a superficial orbital dermoid cyst. Magnetic resonance imaging (MRI) was deemed unnecessary due to the absence of deep orbital involvement or neurological signs.
Diagnosis
Based on the clinical presentation and radiological findings, a provisional diagnosis of a right periocular dermoid cyst was made. Surgical excision was advised to prevent future complications, alleviate cosmetic concerns, and obtain histopathological confirmation.
Management and Outcome
Multidisciplinary Approach
The patient was managed through a multidisciplinary team involving ophthalmology, pediatric surgery, radiology, anesthesiology, and pathology. Detailed counseling was provided to the caregivers regarding the benign nature of the lesion, surgical procedure, potential complications, risk of recurrence, and expected cosmetic outcome.
Therapeutic Management
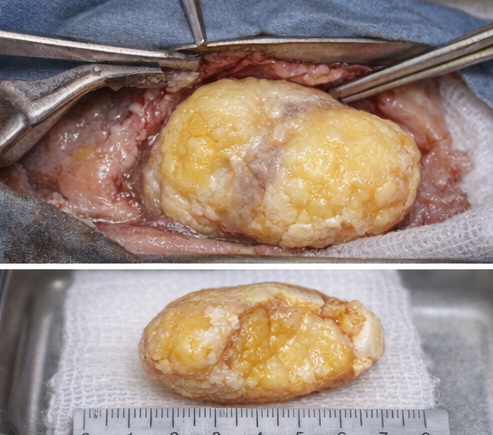
The child underwent elective surgical excision under general anesthesia. A lateral eyebrow incision was chosen to provide optimal exposure while ensuring a cosmetically favorable scar. Intraoperatively, a well-encapsulated cystic mass was identified along the frontozygomatic suture. The cyst contained thick, yellowish, keratinous material consistent with a dermoid cyst.
Careful blunt and sharp dissection was performed to excise the lesion completely without rupture. The surrounding orbital structures, including the lacrimal gland and extraocular muscles, were preserved. Hemostasis was achieved, and the wound was closed in layers.
Histopathological Findings
Histopathological examination of the excised specimen revealed a cyst lined by stratified squamous epithelium containing laminated keratin. The cyst wall showed adnexal structures including sebaceous glands and hair follicles. There was no evidence of cellular atypia, dysplasia, or malignancy, confirming the diagnosis of a dermoid cyst.
Follow-Up
The postoperative period was uneventful. The patient was discharged on the first postoperative day with instructions for wound care and follow-up. At one-month follow-up, the surgical site had healed well with minimal scarring. There was no evidence of infection, inflammation, or recurrence.
Subsequent follow-up visits at three months and six months revealed no recurrence of the lesion. Visual acuity and ocular motility remained normal, and the cosmetic outcome was satisfactory. The caregivers expressed satisfaction with the surgical result.

Discussion
Dermoid cysts of the orbit are benign congenital lesions that typically present in childhood and account for a significant proportion of pediatric orbital masses. Their predilection for orbital suture lines reflects their embryological origin. Superficial dermoid cysts often present early and are easily diagnosed clinically, whereas deeper lesions may present later with proptosis or ocular displacement [3].
Imaging is crucial in preoperative evaluation to determine lesion depth and extension. CT scanning is particularly valuable due to its ability to detect fat density and associated bony changes, while MRI provides superior soft tissue contrast in cases of suspected intracranial extension [4].
Complete surgical excision is the treatment of choice and is curative in the majority of cases. Meticulous dissection is essential to avoid rupture, as spillage of cyst contents can lead to intense inflammatory reactions and increase the risk of recurrence. Early surgical intervention is often recommended to prevent progressive enlargement and cosmetic deformity.
Conclusion
Dermoid cyst should be considered a primary differential diagnosis in congenital or long-standing periocular swellings in pediatric patients. A structured diagnostic approach involving detailed clinical examination, appropriate imaging, and histopathological confirmation is essential for accurate diagnosis and effective management. Multidisciplinary coordination and timely surgical excision result in excellent functional and cosmetic outcomes, with minimal risk of recurrence.
References
- Shields JA, Shields CL. Orbital cysts of childhood: classification, clinical features, and management. Surv Ophthalmol. 2004;49(3):281–299.
- Rootman J. Diseases of the Orbit: A Multidisciplinary Approach. 2nd ed. Lippincott Williams & Wilkins; 2003.
- Bonavolontà G, et al. Dermoid cysts: 16-year survey. Ophthal Plast Reconstr Surg. 1995;11(3):187–192.
- Mafee MF, et al. Imaging of orbital and visual pathway lesions. Radiol Clin North Am. 1999;37(1):169–191.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Examines Office-Based Transperineal Prostate Biopsies Methodology.
2.
A global study demonstrates that screening for lung cancer significantly raises the long-term survival rate.
3.
Is a $2,000 Whole-Body MRI Worth It?
4.
Surgery may not be necessary to treat invasive breast cancer
5.
Limited Benefit from New Drugs; Significant Increase in Drug Prices; AI Boost for Mammo Results.
1.
Understanding Evans Syndrome: Causes, Symptoms, and Treatment Options
2.
Understanding Sepsis and Precision-Medicine-Based Immunotherapy: A Pathophysiological Perspective
3.
Exploring The Science Of Hematopoietic Stem Cell Transplantation: What You Need To Know
4.
Unlocking the Secret to Accurate ANC Calculation with This Informative Blog Post
5.
Understanding Lymphedema: Symptoms, Causes, and Treatment
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Pazopanib: A Game-Changer in Managing Advanced Renal Cell Carcinoma - Part VI
2.
Rates of CR/CRi and MRD Negativity in Iontuzumab-Treated Patients
3.
Management of 1st line ALK+ mNSCLC (CROWN TRIAL Update) - Part II
4.
First-Line Maintenance Therapy for Metastatic Urothelial Carcinoma: Bridging Clinical Practice and Trials
5.
Recent Data Analysis for First-Line Treatment of ALK+ NSCLC: A Final Discussion

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge