COVID-19–Associated Mucormycosis Following Corticosteroid Overuse: Clinical Presentation, Diagnostic Challenges, and Multidisciplinary Management - A Case Report
OthersPage Navigation
Abstract
Coronavirus disease 2019 (COVID-19) has been associated with a surge in secondary opportunistic infections, particularly mucormycosis, during and after recovery. Mucormycosis is an aggressive, angioinvasive fungal infection caused by fungi of the order Mucorales, predominantly affecting immunocompromised individuals. Excessive or inappropriate corticosteroid use during COVID-19 treatment, especially in patients with diabetes mellitus, has been identified as a major precipitating factor.
We report a case of rhino-orbital-cerebral mucormycosis in a middle-aged patient with uncontrolled diabetes mellitus following recovery from COVID-19 pneumonia treated with high-dose systemic corticosteroids. This case highlights the clinical features, diagnostic approach, imaging findings, therapeutic challenges, and outcomes, emphasizing the importance of judicious steroid use and early multidisciplinary intervention.
Introduction
Mucormycosis, commonly referred to as “black fungus,” is a rare but life-threatening opportunistic fungal infection characterized by rapid tissue invasion and high mortality. The disease is caused by filamentous fungi belonging to the order Mucorales, including Rhizopus, Mucor, and Rhizomucor species. These organisms are ubiquitous in the environment and typically pose little risk to immunocompetent individuals.
During the COVID-19 pandemic, a marked increase in cases of mucormycosis was reported, particularly in low- and middle-income countries. The convergence of risk factors such as uncontrolled diabetes mellitus, COVID-19–induced immune dysregulation, and widespread use of systemic corticosteroids created a favorable milieu for fungal proliferation. Corticosteroids, while lifesaving in hypoxic COVID-19 patients, can exacerbate hyperglycemia, impair neutrophil function, and suppress cellular immunity, thereby increasing susceptibility to invasive fungal infections.
Rhino-orbital-cerebral mucormycosis (ROCM) is the most common clinical form seen in COVID-19–associated cases and often presents with sinonasal symptoms that rapidly progress to orbital and intracranial involvement. Early recognition and prompt treatment are critical to improve survival. This case report describes a typical presentation of post-COVID mucormycosis associated with steroid overuse and outlines diagnostic and therapeutic considerations.
Case Report
Patient History
A 52-year-old man presented to the otorhinolaryngology emergency department with complaints of left-sided facial pain, nasal congestion, and swelling around the left eye for 5 days. He also reported headache, fever, and blackish nasal discharge over the preceding 2 days.
The patient had recovered from moderate-to-severe COVID-19 pneumonia 3 weeks prior. During hospitalization, he received supplemental oxygen and high-dose intravenous corticosteroids (dexamethasone 12 mg/day for 10 days), followed by oral steroids continued at home for an additional week without medical supervision.
He was a known case of type 2 diabetes mellitus for 10 years, with poor glycemic control and irregular follow-up. There was no history of malignancy, organ transplantation, or prior fungal infections.
Clinical Examination
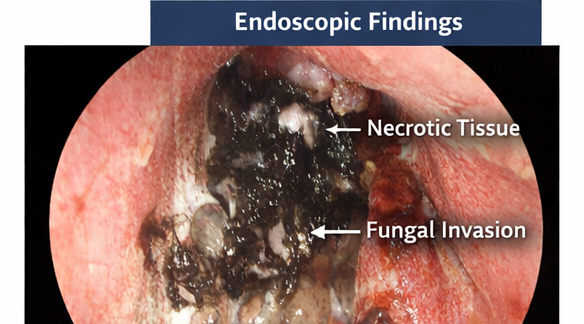
On examination, the patient appeared ill and febrile. Facial inspection revealed periorbital edema and erythema on the left side, with mild ptosis. Nasal examination showed black necrotic eschar over the left inferior turbinate and septum. Oral cavity inspection revealed palatal discoloration with ulceration.

Ophthalmological evaluation demonstrated reduced visual acuity in the left eye, restricted extraocular movements, and mild proptosis. Neurological examination revealed no focal deficits. Vital signs were stable, and systemic examination was otherwise unremarkable.
Clinical Evaluation
Differential Diagnosis
Based on the clinical presentation and risk factors, the following differential diagnoses were considered:
• Rhino-orbital-cerebral mucormycosis
• Acute invasive fungal sinusitis
• Bacterial orbital cellulitis
• Cavernous sinus thrombosis
• Sinonasal malignancy
The presence of necrotic nasal tissue, recent COVID-19 infection, uncontrolled diabetes, and corticosteroid overuse strongly favored a diagnosis of mucormycosis.
Investigations
Laboratory Studies
Laboratory evaluation revealed markedly elevated fasting plasma glucose (286 mg/dL) and HbA1c of 10.1%, indicating poor glycemic control. Serum ferritin levels were elevated. Complete blood count showed leukocytosis with neutrophilia. Renal and liver function tests were within normal limits.
Radiological Imaging
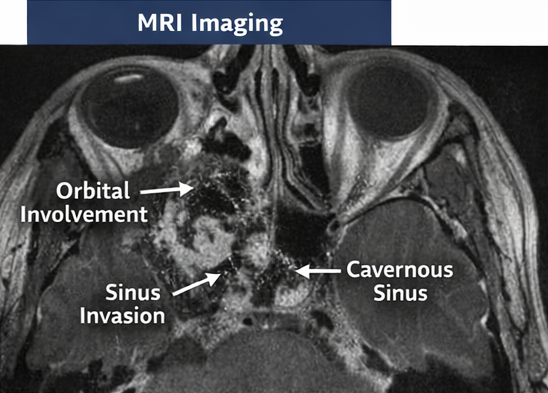
Contrast-enhanced magnetic resonance imaging (MRI) of the paranasal sinuses and orbit demonstrated mucosal thickening of the left maxillary, ethmoid, and sphenoid sinuses with areas of non-enhancement suggestive of tissue necrosis. There was extension into the left orbit with involvement of the medial rectus muscle and early signs of cavernous sinus involvement.
Microbiological and Histopathological Evaluation
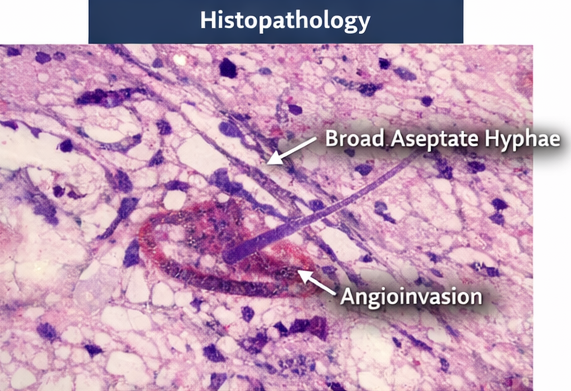
Endoscopic nasal biopsy specimens revealed broad, aseptate hyphae with right-angle branching on potassium hydroxide (KOH) mount. Histopathological examination using hematoxylin and eosin staining confirmed angioinvasive fungal elements consistent with mucormycosis. Fungal culture later identified Rhizopus species.
Diagnosis
A definitive diagnosis of COVID-19–associated rhino-orbital-cerebral mucormycosis was established based on clinical features, imaging findings, and microbiological confirmation in the setting of uncontrolled diabetes and recent corticosteroid overuse.
Management and Outcome
Therapeutic Management
The patient was immediately started on intravenous liposomal amphotericin B at a dose of 5 mg/kg/day. Strict glycemic control was achieved using intravenous insulin infusion under endocrinology supervision. Corticosteroids were discontinued.
Urgent functional endoscopic sinus surgery (FESS) with extensive surgical debridement of necrotic tissue was performed. Intraoperatively, extensive fungal involvement of the maxillary and ethmoid sinuses was noted.
A multidisciplinary team involving otorhinolaryngology, infectious disease specialists, ophthalmology, endocrinology, and critical care managed the patient throughout hospitalization.
Outcome
The patient showed gradual clinical improvement with reduction in facial pain and orbital swelling over 10 days. Visual acuity stabilized without further deterioration. He completed a 4-week course of liposomal amphotericin B, followed by step-down therapy with oral posaconazole.
At 3-month follow-up, the patient remained clinically stable with no evidence of disease recurrence. Glycemic control improved significantly with regular follow-up and adherence to treatment.
Discussion
COVID-19–associated mucormycosis has emerged as a serious complication, particularly in patients with diabetes mellitus exposed to systemic corticosteroids. Steroids impair phagocytic function, induce hyperglycemia, and increase free iron levels, all of which facilitate fungal growth and invasion.
Rhino-orbital-cerebral involvement is the most frequent manifestation and carries a high risk of morbidity and mortality if not promptly treated. Early symptoms are often subtle and nonspecific, leading to diagnostic delays. The presence of black necrotic tissue is a hallmark but may appear late in the disease course.
Management requires a combination of early antifungal therapy, aggressive surgical debridement, and correction of underlying metabolic abnormalities. Liposomal amphotericin B remains the treatment of choice, while newer azoles such as posaconazole and isavuconazole are used as step-down or salvage therapy.
This case underscores the importance of rational corticosteroid use during COVID-19 treatment and highlights the need for vigilance in high-risk patients during the post-COVID recovery period.
Conclusion
Mucormycosis is a devastating opportunistic infection that has gained prominence during the COVID-19 pandemic, largely driven by corticosteroid overuse and uncontrolled diabetes mellitus. Early clinical suspicion, prompt diagnostic evaluation, and aggressive multidisciplinary management are essential to improve outcomes. Preventive strategies, including judicious steroid prescribing and optimal glycemic control, remain critical to reducing disease burden.
References
- Cornely OA, et al. Global guideline for the diagnosis and management of mucormycosis. Lancet Infect Dis. 2019;19(12):e405–e421.
- John TM, et al. COVID-19–associated mucormycosis: a serious threat. Clin Microbiol Infect. 2021;27(5):e1–e7.
- Spellberg B, et al. Mucormycosis: pathogenesis, clinical manifestations, and management. Clin Infect Dis. 2005;41(5):634–653.
- Sen M, et al. Epidemiology, clinical profile, and outcome of COVID-19–associated mucormycosis. Mycoses. 2021;64(9):1015–1029.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Remote monitoring can improve recovery from cancer surgery
2.
Intractable cancers may respond better to treatment when using new radiation and high-performance computing.
3.
A Win for AI in Cancer; 2025's Transformative Drugs; FDA Clarifies 'Underway' Trials
4.
Conditional EU Nod for Weekly Pill in Pediatric Glioma
5.
high response rate when using a bispecific antibody to treat R/R multiple myeloma.
1.
The Technological Revolution in Precision Oncology and Tumor Microenvironment Therapy
2.
The Role of the Oncology Pharmacist: From Treatment to Trials and Beyond
3.
Unlocking the Secrets of Neutrophils: Exploring Their Role in Immune Defense
4.
New Hope for Rectal Cancer Patients: Breakthrough Drug Shows Promising Results
5.
Unveiling the Mystery of Echinocyte: A Closer Look at the Unique Red Blood Cell
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Role of Nimotuzumab in Management of Nasopharyngeal Cancer
2.
The Landscape of First-Line Treatment for Urothelial Carcinoma- The Conclusion
3.
Pazopanib Takes Center Stage in Managing Renal Cell Carcinoma - Part III
4.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part IV
5.
An Eagles View - Evidence-based Discussion on Iron Deficiency Anemia- Panel Discussion

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge