Hegar’s Sign as an Early Clinical Indicator of Pregnancy: A Case Report
OthersPage Navigation
Abstract
Hegar’s sign refers to the softening and compressibility of the lower uterine segment and is a well-recognized early clinical sign of pregnancy. It typically appears between the sixth and eighth weeks of gestation and reflects physiological changes in uterine vascularity and tissue consistency. We report the case of a 26-year-old woman who presented with amenorrhea and nonspecific lower abdominal discomfort. Pelvic examination revealed a softened lower uterine segment consistent with Hegar’s sign, raising clinical suspicion of early pregnancy. Subsequent laboratory testing and ultrasonography confirmed an early intrauterine pregnancy. This case highlights the continued clinical relevance of careful bimanual examination and recognition of classical physical signs in the early diagnosis of pregnancy, particularly in resource-limited or primary care settings.
Introduction
Early diagnosis of pregnancy is essential for the initiation of appropriate antenatal care, effective patient counseling, and the timely identification and management of potential maternal or fetal complications. Prompt recognition allows for early nutritional supplementation, lifestyle modification, risk stratification, and planning of necessary investigations. Although biochemical assays and ultrasonography are now widely available and form the cornerstone of pregnancy confirmation, classical clinical signs continue to hold significant value in early gestational assessment, particularly during the initial clinical encounter or in settings where immediate access to advanced diagnostics may be limited [1]. Careful history-taking and thorough physical examination remain fundamental components of obstetric practice.
Hegar’s sign, first described by Ernst Ludwig Alfred Hegar in the late nineteenth century, is a well-recognized early clinical sign of pregnancy. It is characterized by softening and compressibility of the lower uterine segment, producing a perceived separation between the relatively firm cervix and the uterine body on bimanual pelvic examination [2]. This physical finding typically becomes appreciable between 6 and 8 weeks of gestation and reflects underlying physiological changes, including increased uterine vascularity, stromal edema, and hormonal influences on smooth muscle and connective tissue architecture [3]. These changes collectively lead to reduced tissue resistance in the uterine isthmus, enabling the examiner to appreciate the characteristic softness.
Although Hegar’s sign is not diagnostic when considered in isolation, it represents an important component of the group of probable signs of pregnancy. When interpreted in conjunction with other clinical findings, patient history, and preliminary investigations, it can raise a strong index of suspicion and guide clinicians toward appropriate confirmatory testing. This case report describes a typical presentation of early pregnancy in which recognition of Hegar’s sign played a pivotal role in initial clinical assessment, emphasizing the continued relevance of classical obstetric examination skills in modern clinical practice.
Case Report
Patient History
A 26-year-old woman presented to the gynecology outpatient clinic with a complaint of missed menstrual period for six weeks. She also reported mild lower abdominal discomfort and breast tenderness for the past ten days. There was no history of vaginal bleeding, severe abdominal pain, or syncope.
Her menstrual cycles were previously regular, occurring every 28–30 days. She had no history of contraceptive use in the preceding three months and was sexually active with her spouse. There was no past history of pelvic inflammatory disease, ectopic pregnancy, or gynecological surgery. Her medical and surgical histories were unremarkable.
Clinical Findings
On general examination, the patient was stable, afebrile, and hemodynamically normal. Abdominal examination revealed no tenderness or guarding.
Pelvic examination showed a soft, bluish cervix without discharge or bleeding. On bimanual examination, the uterus was slightly enlarged and anteverted. Notably, the lower uterine segment was markedly softened and compressible between the examining fingers, giving the characteristic impression of separation between the cervix and uterine body. This finding was consistent with Hegar’s sign and suggested early pregnancy [2,3].

No adnexal tenderness or masses were appreciated.
Investigations
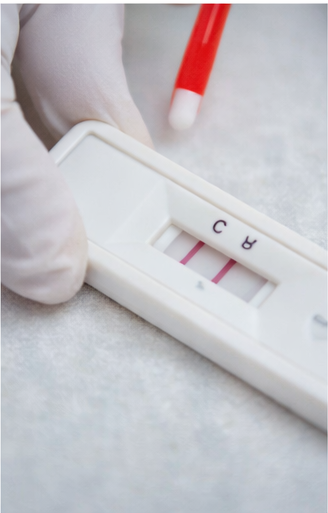
A urine pregnancy test was positive, providing an initial indication of pregnancy.
Subsequent quantitative assessment of serum beta–human chorionic gonadotropin (β-hCG) levels revealed values elevated in a pattern consistent with early gestation, supporting the clinical suspicion.
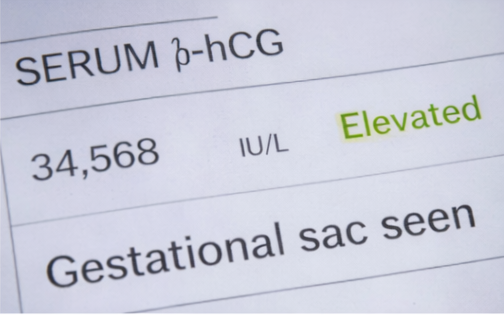
Transvaginal ultrasonography further confirmed the diagnosis by demonstrating a small intrauterine gestational sac corresponding to approximately six weeks of gestation.
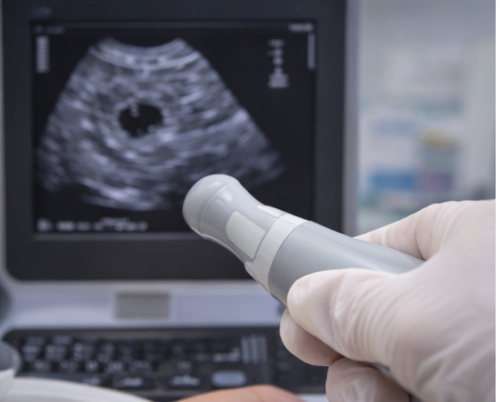
No fetal or maternal abnormalities were identified at this stage, and there was no evidence of adnexal pathology or free pelvic fluid, effectively excluding ectopic pregnancy or other acute pelvic conditions.
Routine laboratory investigations were conducted as part of the initial antenatal evaluation. These included a complete blood count and urinalysis, both of which were within normal limits, indicating the absence of anemia, infection, or urinary abnormalities. The normal laboratory findings, in conjunction with imaging and hormonal assessment, supported an uncomplicated early intrauterine pregnancy at presentation..
Management and Outcome
The patient was counseled in detail regarding the confirmation of an early intrauterine pregnancy and informed about the expected physiological changes during early gestation. She was educated on the importance of routine antenatal care, including timely investigations, scheduled follow-up visits, and adherence to prescribed supplements. Folic acid supplementation was initiated to support neural tube development, and guidance was provided on appropriate lifestyle modifications, balanced nutritional intake, adequate rest, and avoidance of potential teratogens.

She was also advised about common warning signs such as abdominal pain, vaginal bleeding, dizziness, or excessive vomiting that would warrant immediate medical attention.
At a follow-up visit two weeks later, the patient remained asymptomatic with no reported complications. Repeat ultrasonography confirmed a viable intrauterine pregnancy with appropriate gestational progression and reassuring fetal parameters for the corresponding gestational age. Based on these findings, she was formally enrolled for regular antenatal follow-up, with a planned schedule for ongoing monitoring, routine screening, and continued prenatal counseling to support optimal maternal and fetal outcomes.
Discussion
Hegar’s sign is one of the classical probable signs of pregnancy and reflects physiological softening of the lower uterine segment due to hormonal influences, particularly progesterone, and increased uterine vascularity [3]. It is typically detectable between the sixth and eighth weeks of gestation and is elicited during bimanual pelvic examination.
Although modern diagnostic tools such as serum β-hCG assays and ultrasonography provide definitive confirmation, recognition of Hegar’s sign remains clinically relevant. It is particularly useful in early presentations, in settings with limited access to imaging, or when laboratory confirmation is pending [4].
The differential diagnosis for uterine softening includes pelvic congestion and uterine pathology; therefore, Hegar’s sign should not be used in isolation to diagnose pregnancy [5]. Instead, it should prompt appropriate confirmatory testing, as demonstrated in this case.
Continued emphasis on physical examination skills is essential in medical training, as classical signs such as Hegar’s sign enhance clinical reasoning and support early diagnosis and patient counseling.
Conclusion
Hegar’s sign remains an important early clinical indicator of pregnancy, reflecting characteristic physiological softening of the lower uterine segment during early gestation. This sign, typically elicited on bimanual examination, results from increased vascularity and hormonal influences on the uterine tissues in the first trimester.
This case highlights the continued clinical relevance of a thorough pelvic examination in raising early suspicion of pregnancy, particularly in settings where access to immediate laboratory testing or imaging may be limited. Recognition of Hegar’s sign can prompt timely further evaluation, including biochemical testing and ultrasonography, before definitive diagnostic confirmation is obtained.
Awareness and correct interpretation of classical obstetric signs, when integrated with modern diagnostic modalities, facilitate early diagnosis, enable prompt initiation of appropriate antenatal care, and contribute to improved maternal and fetal outcomes.
References
-
Cunningham FG, Leveno KJ, Bloom SL, et al. Williams Obstetrics. 25th ed. McGraw-Hill; 2018.
-
Hegar E. Beiträge zur Pathologie des Eies und zur Frühdiagnose der Schwangerschaft. Arch Gynäkol. 1884;25:1–15.
-
Hacker NF, Gambone JC, Hobel CJ. Hacker & Moore’s Essentials of Obstetrics and Gynecology. 6th ed. Elsevier; 2016.
-
Berek JS. Berek & Novak’s Gynecology. 16th ed. Wolters Kluwer; 2020.
-
DeCherney AH, Nathan L, Laufer N, Roman AS. Current Diagnosis & Treatment: Obstetrics & Gynecology. 12th ed. McGraw-Hill; 2019.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
According to the CAPTIVATE Study, fixed-duration ibrutinib plus venetoclax may be beneficial for patients with high-risk chronic lymphocytic leukemia.
2.
Scientists develop novel adjuvant delivery system to enhance cancer vaccine effectiveness
3.
Vepdegestrant Earns FDA Nod for ESR1-Mutated Breast Cancer
4.
According to a study, taking part in a clinical trial for cancer may not actually increase survival.
5.
A new blood test greatly increases the ability to detect cancer.
1.
Cancer Memory: A Persistent Threat to Tumor Recurrence and Metastasis
2.
Unraveling the Mysteries of Hematocrit: How It Impacts Your Health
3.
The Transformative Power of Genomics in the Diagnosis and Management of Rare Cancers
4.
Omega-3 Fatty Acids as Molecular Adjuvants Against Chemoresistance in Breast Cancer
5.
Surprising Symptoms of Prostate Cancer: What You Need to Know
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Navigating the Complexities of Ph Negative ALL - Part X
2.
Efficient Management of First line ALK-rearranged NSCLC - Part III
3.
What Therapy Would Yield the Best Outcomes In Patients with R/R B-cell ALL?
4.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part IV
5.
Updates on Standard V/S High Risk Myeloma Treatment- The Next Part

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge