Needle Stick Injury: Clinical Evaluation, Multidisciplinary Management, and Outcome - A Case Report
OthersPage Navigation
Abstract
Needle stick injury (NSI) is a common occupational hazard among healthcare workers and poses a significant risk for transmission of blood-borne pathogens, including hepatitis B virus, hepatitis C virus, and human immunodeficiency virus. Such injuries often occur during routine clinical procedures and may be underestimated despite their potential physical, psychological, and medico-legal consequences. Prompt risk assessment, appropriate post-exposure prophylaxis, and structured follow-up are critical to minimizing infection risk and ensuring healthcare worker safety. We report a case of accidental needle stick injury in a hospital nurse during venipuncture, detailing the clinical evaluation, immediate management, multidisciplinary involvement, and outcome. This case highlights the importance of institutional protocols, early intervention, and preventive strategies in managing occupational exposures.
Introduction
Needle stick injury is defined as accidental penetration of the skin by a needle or other sharp medical device contaminated with blood or body fluids. It represents a major occupational health concern in healthcare settings worldwide, particularly affecting nurses, physicians, laboratory personnel, and housekeeping staff [1].
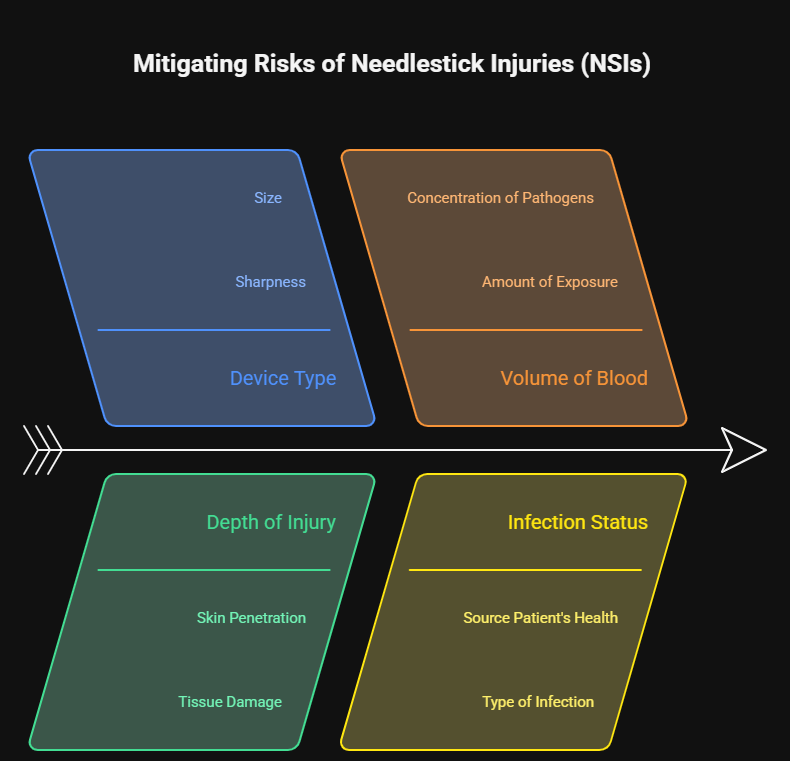
The risk associated with NSI depends on multiple factors, including the type of device, depth of injury, volume of blood involved, and the infection status of the source patient. Although many exposures do not result in infection, the psychological stress and anxiety associated with potential disease transmission can be substantial [2]. Early reporting, systematic evaluation, and adherence to post-exposure protocols are essential to mitigate risks.
This case report describes the evaluation and management of a needle stick injury in a tertiary care hospital, emphasizing multidisciplinary coordination and preventive measures.
Case Report
Patient History
A 29-year-old female staff nurse working in the medical ward sustained a needle stick injury while performing routine venipuncture on an admitted patient. The injury occurred when the patient moved suddenly during blood collection, causing the used hollow-bore needle to puncture the nurse’s thumb.

The nurse immediately noticed mild bleeding at the puncture site. She had no prior history of occupational exposure, was otherwise healthy, and had completed the hepatitis B vaccination series five years earlier. There was no history of immunocompromising conditions.
Immediate First Aid
The affected area was immediately washed with soap and running water. The nurse did not attempt to squeeze the wound excessively or apply antiseptic solutions locally. She promptly reported the incident to the hospital infection control unit as per institutional protocol.

Clinical Evaluation
Source Patient Assessment
The source patient was a 54-year-old male admitted for evaluation of chronic liver disease. After obtaining informed consent, blood samples were collected from the source patient for hepatitis B surface antigen, anti-hepatitis C virus antibodies, and human immunodeficiency virus testing.
Exposed Healthcare Worker Assessment
Baseline investigations for the exposed nurse included hepatitis B surface antigen, anti-hepatitis C virus antibodies, and human immunodeficiency virus serology. Hepatitis B antibody titers were also assessed to evaluate immune status.
Investigations
Laboratory Studies
Baseline serological tests for the nurse were negative for hepatitis B, hepatitis C, and human immunodeficiency virus. Hepatitis B surface antibody levels were found to be protective. The source patient tested positive for hepatitis C virus antibodies but was negative for hepatitis B surface antigen and human immunodeficiency virus.

Diagnosis
A diagnosis of occupational needle stick injury with potential exposure to hepatitis C virus was established based on the nature of the injury and source patient serology.
Management and Outcome
Multidisciplinary Approach
The case was managed collaboratively by the infection control team, occupational health department, internal medicine, and hospital administration. Counseling was provided to address anxiety and explain the risk of transmission and follow-up plan.
Therapeutic Management
As there is no approved post-exposure prophylaxis for hepatitis C virus, no antiviral therapy was initiated. The nurse was reassured regarding the relatively low risk of transmission. No post-exposure prophylaxis was required for hepatitis B due to documented immunity, and none was indicated for human immunodeficiency virus as the source patient tested negative.
The nurse was advised to report any symptoms suggestive of acute viral illness and to avoid blood donation during the follow-up period.
Follow-Up
Serial follow-up testing for hepatitis C virus was scheduled at 6 weeks, 3 months, and 6 months post-exposure. All follow-up serological tests remained negative. The nurse did not develop any clinical symptoms and continued her duties without restriction.
Discussion
Needle stick injuries remain a persistent occupational risk despite advances in safety-engineered devices and infection control practices. Hollow-bore needles, deep injuries, high viral load in the source patient, and delayed reporting significantly increase the risk of transmission of blood-borne pathogens such as hepatitis B, hepatitis C, and human immunodeficiency virus [3]. High-risk clinical settings, including emergency departments and intensive care units, further contribute to the incidence of such injuries due to time pressure and frequent invasive procedures.
This case underscores the importance of immediate first aid, prompt reporting, and structured evaluation following NSI. A multidisciplinary approach ensures comprehensive risk assessment, timely initiation of post-exposure measures, appropriate counseling, and strict adherence to follow-up protocols. Psychological support is an essential component of care, as anxiety, fear of seroconversion, and concerns regarding professional and personal implications often outweigh the actual risk of infection [4].
Prevention remains the cornerstone of NSI management and includes regular staff training, strict adherence to standard precautions, use of safety-engineered devices, avoidance of needle recapping, and fostering a strong culture of safety and accountability within healthcare institutions.
Conclusion
Needle stick injury is a preventable yet significant occupational hazard in healthcare settings. Early recognition, immediate first aid, systematic risk assessment, and multidisciplinary management are critical to minimizing the risk of blood-borne pathogen transmission and addressing the psychological impact on healthcare workers. This case highlights the effectiveness of institutional protocols and coordinated care in achieving favorable outcomes. Ongoing education, adherence to standard precautions, and implementation of preventive strategies are essential to reduce the incidence of needle stick injuries and safeguard healthcare professionals.
References
- World Health Organization. Aide-memoire for a strategy to protect health workers from infection with bloodborne viruses. WHO; 2017.
- Tarantola A, et al. Infection risks following accidental exposure to blood or body fluids in health care workers: a review of pathogens transmitted in published cases. Am J Infect Control. 2006;34(6):367–375.
- Prüss-Üstün A, et al. Sharps injuries: global burden of disease from sharps injuries to health-care workers. WHO Environmental Burden of Disease Series. 2003.
- Trim JC, Elliott TS. A review of sharps injuries and preventative strategies. J Hosp Infect. 2003;53(4):237–242.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Sub-Q Ketamine is Safe and Very Effective for Severe Depression.
2.
Study indicates that exercise can help colon cancer survivors live as long as matched individuals
3.
Contradictory Results Are Found in Two Pembrolizumab Trials for Head and Neck Cancer.
4.
Can Concurrent Boost Safely Shorten Breast Cancer Radiation?
5.
Positive Trials; Malignancies Increasing in Younger Adults; Andre Braugher's Cancer Dx.
1.
Trends in Incidence, Care, and Surgery for Medullary Thyroid Cancer: A Review
2.
Antibody-Drug Conjugates in Oncology: Breakthroughs, Clinical Updates, and Pipeline Innovation
3.
Navigating the Stages of Thyroid Cancer: A Guide for Patients
4.
Polycythemia Vera: A Historical Perspective and Contemporary Management
5.
Glofitamab: A Breakthrough Therapy for Relapsed/Refractory Mantle Cell Lymphoma
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Pazopanib: A Game-Changer in Managing Advanced Renal Cell Carcinoma - Part IV
2.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VIII
3.
Evolving Space of First-Line Treatment for Urothelial Carcinoma- Case Discussion
4.
Key Takeaways from The CROWN Trial For ALK + NSCLC Patients with CNS Diseases
5.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part I

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge