DRESS Syndrome Following Antibiotic Treatment for Urinary Tract Infection: A Case Report
OthersPage Navigation
Abstract
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) syndrome is a rare, potentially life-threatening severe cutaneous adverse drug reaction characterized by extensive skin eruption, fever, hematologic abnormalities, lymphadenopathy, and internal organ involvement [1]. We report a case of DRESS syndrome in a 27-year-old female who developed high-grade fever, diffuse pruritic rash, facial edema, lymphadenopathy, eosinophilia, and hepatic dysfunction following initiation of a new antibiotic for a urinary tract infection. Prompt recognition, withdrawal of the offending drug, and initiation of systemic corticosteroid therapy resulted in clinical improvement. This case highlights the importance of early diagnosis of DRESS syndrome to reduce morbidity and prevent fatal complications.
Introduction
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) syndrome, also known as drug-induced hypersensitivity syndrome (DIHS), is a severe idiosyncratic drug reaction with a delayed onset, typically occurring 2–8 weeks after exposure to the offending medication [1,2]. The syndrome is characterized by a constellation of features including fever, widespread cutaneous eruption, facial edema, hematologic abnormalities such as eosinophilia or atypical lymphocytosis, lymphadenopathy, and involvement of internal organs, most commonly the liver [3].
A wide range of medications have been implicated in DRESS syndrome, including anticonvulsants, sulfonamides, allopurinol, and antibiotics commonly used for urinary tract infections [2,4]. The pathogenesis is complex and multifactorial, involving drug-specific immune responses, genetic susceptibility, and viral reactivation, particularly human herpesvirus-6 (HHV-6) [3,5].
Given its variable presentation and overlap with other dermatologic and systemic conditions, DRESS syndrome is frequently underrecognized or misdiagnosed. Delay in diagnosis can result in severe complications, including fulminant hepatitis, renal failure, myocarditis, and mortality rates reported up to 10% [1,6]. Early identification and prompt discontinuation of the offending drug are therefore critical for favorable outcomes.
Case Report
Patient History
A 27-year-old female presented to the emergency department with a 4-day history of high-grade fever, generalized pruritus, and progressive skin rash. Two weeks prior, she had been started on a new oral antibiotic for an uncomplicated urinary tract infection. The patient reported initial improvement in urinary symptoms but subsequently developed fever followed by a rapidly spreading itchy rash.


She denied any prior history of drug allergies, autoimmune disease, or recent viral infections. There was no history of similar episodes in the past. She reported malaise and facial swelling but denied shortness of breath or mucosal involvement.
Clinical Findings
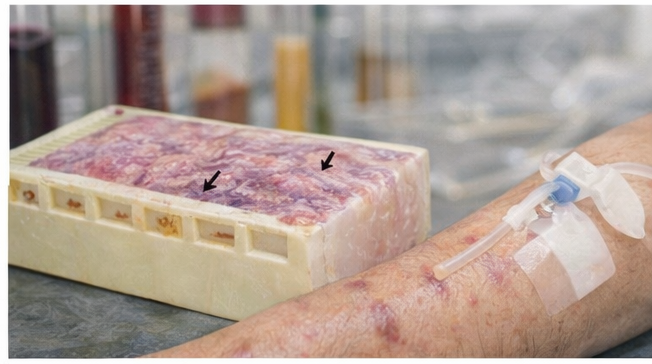
On examination, the patient was febrile with a temperature of 39°C. Cutaneous examination revealed a diffuse morbilliform rash involving the trunk and extremities, interspersed with papules, targetoid lesions, and scattered vesicles and blisters. Marked facial edema, particularly involving the periorbital region, was noted.

The rash was intensely pruritic but non-tender. No epidermal detachment was observed. Mucous membranes were spared. Examination revealed significant bilateral inguinal lymphadenopathy, with nodes that were enlarged, firm, and mildly tender. There was no hepatosplenomegaly on abdominal examination.
These findings raised strong clinical suspicion for a severe cutaneous adverse drug reaction, particularly DRESS syndrome [1,3].
Investigations
Laboratory evaluation revealed leukocytosis with marked eosinophilia (absolute eosinophil count: 2,100 cells/µL). Liver function tests showed elevated transaminases (AST and ALT approximately three times the upper limit of normal), consistent with hepatic involvement. Renal function tests were within normal limits.
Serologic testing for viral hepatitis was negative. Blood cultures were sterile. Skin biopsy demonstrated interface dermatitis with eosinophilic infiltrates, supporting a drug-induced hypersensitivity reaction. Based on the RegiSCAR scoring system, a diagnosis of definite DRESS syndrome was established [4,6].
Management and Outcome
The suspected offending antibiotic was immediately discontinued. The patient was initiated on systemic corticosteroid therapy (oral prednisolone 1 mg/kg/day), along with antihistamines and supportive care. Close monitoring of liver function tests and complete blood counts was undertaken.
Over the following week, the patient showed marked clinical improvement, with resolution of fever, gradual reduction in facial edema, and fading of the rash. Eosinophil counts and liver enzymes showed a downward trend. Corticosteroids were slowly tapered over six weeks to prevent relapse.
At 8-week follow-up, the patient had complete resolution of cutaneous lesions and normalization of laboratory parameters, with no evidence of recurrence.
Discussion
DRESS syndrome is a severe and potentially fatal adverse drug reaction characterized by delayed onset and multisystem involvement, typically occurring several weeks after exposure to the offending medication [1,2]. Cutaneous manifestations are polymorphic and may include morbilliform eruptions, targetoid lesions, vesicles, bullae, and prominent facial edema, as observed in this case [3,5]. The rash often begins on the trunk and spreads centrifugally, and intense pruritus is a common feature. Lymphadenopathy and eosinophilia are hallmark findings and are particularly useful in differentiating DRESS syndrome from other drug eruptions such as simple exanthematous reactions or Stevens–Johnson syndrome [1,3].
The liver is the most commonly affected internal organ in DRESS syndrome, with hepatic involvement reported in up to 70–90% of cases, and it remains a major determinant of prognosis and mortality [4,6]. Manifestations range from mild transaminitis to severe hepatitis and, rarely, acute liver failure. Antibiotics used for urinary tract infections, particularly sulfonamides and beta-lactams, are well-documented triggers and are frequently implicated due to their widespread use [2,4]. Recognition of the temporal relationship between drug initiation and symptom onset is therefore critical for early diagnosis.
Early withdrawal of the offending drug significantly improves clinical outcomes and reduces mortality. However, systemic inflammation may persist or even worsen after drug cessation due to ongoing immune activation. Systemic corticosteroids remain the cornerstone of treatment in moderate to severe cases, particularly when there is evidence of internal organ involvement such as hepatitis, nephritis, or pneumonitis [5,6]. Delayed diagnosis, inadequate dosing, or premature tapering of corticosteroids may result in relapse, chronic organ dysfunction, or progression to life-threatening complications, emphasizing the importance of gradual tapering and long-term follow-up to monitor for recurrence and late autoimmune sequelae [6,7].
Conclusion
DRESS syndrome should be strongly suspected in patients presenting with fever, widespread rash, facial edema, lymphadenopathy, eosinophilia, and evidence of internal organ dysfunction following recent drug exposure, particularly when symptoms develop with a delayed onset of several weeks. The clinical presentation may be heterogeneous and evolve over time, making early diagnosis challenging. A high index of suspicion is therefore required, especially in patients who have recently been started on high-risk medications such as antibiotics, anticonvulsants, or allopurinol. Careful assessment of the temporal relationship between drug initiation and symptom onset is a key step in identifying the offending agent and establishing the diagnosis.
Early recognition and prompt discontinuation of the suspected medication are the most critical interventions and are strongly associated with improved outcomes and reduced mortality. Timely initiation of systemic corticosteroids is essential in patients with moderate to severe disease, particularly when there is involvement of vital organs such as the liver, kidneys, lungs, or heart. Supportive care, close clinical monitoring, and serial laboratory evaluation are equally important to detect progression or complications at an early stage.
Clinician awareness of this rare but severe condition is crucial, particularly given the widespread use of medications commonly implicated in DRESS syndrome. Education regarding early warning signs and appropriate referral can facilitate timely management. Long-term follow-up is necessary, as patients remain at risk for delayed relapse, steroid dependence, and the development of autoimmune sequelae such as thyroiditis, type 1 diabetes mellitus, or autoimmune hepatitis. A multidisciplinary approach involving dermatology, internal medicine, and relevant subspecialties can optimize patient outcomes and reduce long-term morbidity [1–7].
References
- Bocquet H, Bagot M, Roujeau JC. Drug-induced pseudolymphoma and drug hypersensitivity syndrome (DRESS). Seminars in Cutaneous Medicine and Surgery. 1996;15(4):250–257.
- Cacoub P, Musette P, Descamps V, et al. The DRESS syndrome: A literature review. American Journal of Medicine. 2011;124(7):588–597.
- Shiohara T, Kano Y. Drug reaction with eosinophilia and systemic symptoms (DRESS): Incidence, pathogenesis and management. Expert Opinion on Drug Safety. 2017;16(2):139–147.
- Kardaun SH, Sidoroff A, Valeyrie-Allanore L, et al. Variability in the clinical pattern of cutaneous side-effects of drugs with systemic symptoms: Does a DRESS syndrome really exist? British Journal of Dermatology. 2007;156(3):609–611.
- Husain Z, Reddy BY, Schwartz RA. DRESS syndrome: Part I. Clinical perspectives. Journal of the American Academy of Dermatology. 2013;68(5):693.e1–693.e14.
- Husain Z, Reddy BY, Schwartz RA. DRESS syndrome: Part II. Management and therapeutics. Journal of the American Academy of Dermatology. 2013;68(5):709.e1–709.e9.
- Chen YC, Cho YT, Chang CY, Chu CY. Drug reaction with eosinophilia and systemic symptoms: A comprehensive review. Journal of Clinical Medicine. 2016;5(11):123.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Charles III, King of Kings, is Cancerous.
2.
Chemo-Free Quadruplet Shows Promise as DLBCL's First Therapy.
3.
Perioperative Anti-PD-1 in Soft-Tissue Sarcoma Boosts Disease-Free Survival
4.
Merck enhances its oncology pipeline by means of a strategic alliance with Hengrui.
5.
WHO releases new R&D landscape analyses highlighting gaps and inequities in cancer research
1.
The benefits and risks of taking fludrocortisone for adrenal insufficiency
2.
Ultimate Guide to Oncology Services in the USA
3.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
4.
Real-World Oncology Insights: CAR-T, Immunotherapy, PROs, and Digital Tools
5.
Introducing the Corrected Calcium Calculator: A Revolutionary Tool in Medical Assessment
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Oropharyngeal Cancer in Relation to HPV Status
2.
Advances in Classification/ Risk Stratification of Plasma Cell Dyscrasias- The Summary
3.
Navigating the Brain Barrier: The CNS Challenge in ALK+ NSCLC
4.
EGFR Mutation Positive Non-Small Cell Lung Cancer- Case Discussion & Conclusion
5.
Management of 1st line ALK+ mNSCLC (CROWN TRIAL Update) - Part V

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge