Ovarian Cyst: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Ovarian cysts are common gynecological conditions encountered in women of reproductive age and are often detected incidentally during routine imaging. They may be functional or pathological in nature and can present with a wide spectrum of clinical manifestations ranging from asymptomatic findings to acute abdominal emergencies. While most ovarian cysts are benign and self-limiting, timely diagnosis and appropriate management are essential to prevent complications such as torsion, rupture, hemorrhage, or malignant transformation. Diagnosis relies on clinical evaluation supported by ultrasonography and, when indicated, advanced imaging and tumor markers. Management strategies are individualized based on patient age, symptomatology, cyst characteristics, and risk of malignancy, and may include observation, medical therapy, or surgical intervention. This case report describes an adult female patient presenting with a symptomatic ovarian cyst, highlighting the clinical features, diagnostic approach, management strategy, and short-term outcomes.
Introduction
Ovarian cysts represent a frequent clinical entity in gynecological practice, particularly among women of reproductive age. They are broadly classified into functional cysts, such as follicular and corpus luteum cysts, and pathological cysts, including endometriomas, dermoid cysts, and neoplastic lesions. Functional cysts arise as part of normal ovulatory physiology and often resolve spontaneously, whereas pathological cysts may persist and require intervention.
Clinical presentation varies widely depending on cyst size, type, and complications. Many cysts remain asymptomatic, while others may present with pelvic pain, menstrual irregularities, abdominal distension, or acute symptoms due to torsion or rupture. Imaging, particularly transvaginal ultrasonography, plays a pivotal role in diagnosis and risk stratification. This case report illustrates the evaluation and management of a symptomatic ovarian cyst in an adult patient, emphasizing a structured, evidence-based approach.
Case Report
Patient History
A 32-year-old female presented to the gynecology outpatient clinic with complaints of intermittent lower abdominal pain for the past two months. The pain was predominantly localized to the left lower abdomen, dull in nature, non-radiating, and occasionally associated with a sensation of pelvic heaviness. The patient also reported mild menstrual irregularity over the preceding three cycles, characterized by delayed menses.

There was no history of acute severe pain, fever, vomiting, abnormal vaginal bleeding, or urinary or bowel disturbances. The patient had no prior gynecological surgeries and no known history of endometriosis or pelvic inflammatory disease. Obstetric history included one full-term normal vaginal delivery. There was no significant family history of gynecological malignancy.
Clinical Examination
General physical examination revealed a hemodynamically stable patient with normal vital signs. Abdominal examination showed mild tenderness in the left lower quadrant without guarding, rigidity, or palpable mass.
On pelvic examination, the uterus was normal in size and anteverted. Left adnexal fullness with mild tenderness was noted, while the right adnexa was unremarkable. No cervical motion tenderness was present.
Clinical Evaluation
Differential Diagnosis
Based on clinical presentation, the differential diagnosis included:
- Functional ovarian cyst
- Endometriotic cyst (endometrioma)
- Benign ovarian neoplasm
- Tubo-ovarian mass
- Pelvic inflammatory disease
Investigations

- Laboratory tests: Complete blood count, renal and liver function tests were within normal limits
- Pregnancy test: Negative
- Tumor markers: Serum CA-125 levels were within normal range
- Ultrasonography: Transvaginal ultrasound revealed a well-defined, unilocular, thin-walled cyst measuring 5.6 × 4.8 cm arising from the left ovary, with clear internal echoes and no solid components or septations
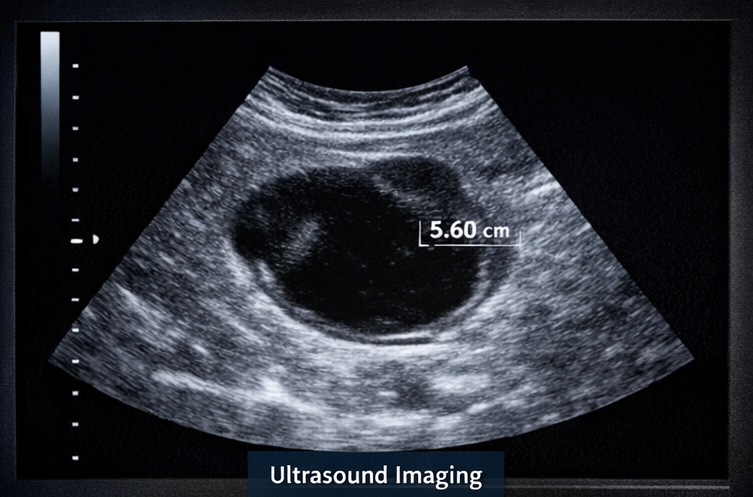
- Color Doppler: Normal vascular flow with no features suggestive of torsion
Based on imaging findings, the cyst was provisionally diagnosed as a benign functional ovarian cyst.
Management and Outcome
Management Strategy
Given the benign appearance of the cyst, moderate size, and absence of acute complications, a conservative approach was adopted:
- Expectant management: Observation with serial follow-up
- Medical therapy: Short course of nonsteroidal anti-inflammatory drugs for pain relief
- Hormonal regulation: Combined oral contraceptive pills prescribed to regulate menstrual cycles and prevent new cyst formation
- Patient counseling: Education regarding symptoms of complications such as acute pain, vomiting, or sudden abdominal distension

Follow-Up and Outcome
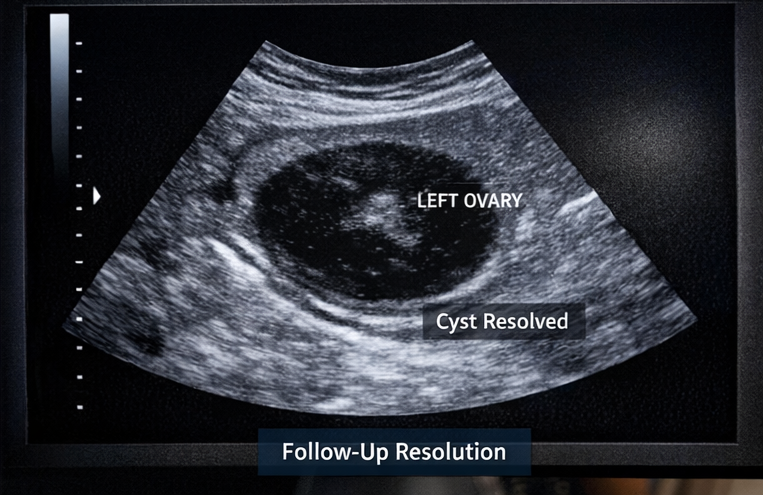
At six-week follow-up, the patient reported significant reduction in abdominal discomfort and normalization of menstrual cycles. Repeat transvaginal ultrasonography demonstrated a marked reduction in cyst size to 2.3 cm.
At three-month follow-up, the cyst had completely resolved on imaging, and the patient remained asymptomatic. No adverse effects of treatment were reported. Continued routine gynecological follow-up was advised.
Discussion
Ovarian cysts are frequently encountered in clinical practice, with the majority being benign and functional in nature. In reproductive-age women, functional cysts commonly arise due to disturbances in normal follicular development and often resolve spontaneously within a few menstrual cycles.
Transvaginal ultrasonography remains the cornerstone of diagnosis, allowing assessment of cyst morphology, size, and features suggestive of malignancy. Tumor markers such as CA-125 may assist in selected cases but have limited specificity in premenopausal women.
Conservative management is appropriate for asymptomatic or mildly symptomatic cysts with benign imaging features. Surgical intervention is reserved for large, persistent, symptomatic, or suspicious lesions, as well as for complications such as torsion or rupture. This case highlights the effectiveness of a conservative, individualized approach in managing a functional ovarian cyst while avoiding unnecessary surgical intervention.
Conclusion
Ovarian cysts are common benign gynecological conditions that frequently present with nonspecific symptoms such as pelvic discomfort, menstrual irregularities, or a sensation of abdominal fullness, and are often detected incidentally during routine pelvic examinations or imaging performed for unrelated indications. Because clinical manifestations can be subtle or overlap with other gynecological conditions, accurate clinical assessment combined with appropriate imaging—particularly transvaginal ultrasonography—is essential for establishing the diagnosis, assessing cyst characteristics, and stratifying the risk of malignancy or complications.
In women of reproductive age, the majority of ovarian cysts demonstrate benign features on imaging and are associated with mild or no symptoms. In such cases, conservative management with careful observation and close follow-up is both safe and effective. This approach allows for spontaneous resolution of functional cysts while minimizing unnecessary interventions and associated morbidity. Serial imaging and clinical monitoring help ensure early detection of changes in cyst size, morphology, or symptomatology that may warrant escalation of care.
Early identification and appropriate management not only alleviate symptoms and improve patient comfort but also reduce the risk of potential complications such as cyst rupture, hemorrhage, or ovarian torsion. Timely counseling and reassurance play an important role in reducing patient anxiety, particularly when cysts are discovered incidentally. A patient-centered approach that integrates thorough clinical evaluation, detailed imaging findings, and individualized treatment planning while considering patient preferences and reproductive goals is fundamental to achieving favorable clinical outcomes and optimizing long-term gynecological health in women with ovarian cysts.
References
- Hoffman, B. L., et al. (2020). Williams Gynecology. McGraw-Hill Education.
- Levine, D., et al. (2010). Management of asymptomatic ovarian and other adnexal cysts imaged at US. Radiology, 256(3), 943–954.
- American College of Obstetricians and Gynecologists. (2016). Practice Bulletin: Evaluation and management of adnexal masses. Obstetrics & Gynecology, 128(5), e210–e226.
- Timmerman, D., et al. (2016). Simple ultrasound-based rules for the diagnosis of ovarian cancer. BMJ, 341, c6839.
- Grimes, D. A., & Hughes, J. M. (1989). Ovarian cysts: Pathogenesis and management. Annals of Internal Medicine, 110(9), 751–761.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Imfinzi + Imjudo, EU approved for patients with advanced lung cancer and non-small cell lung cancer: AstraZeneca
2.
More Support for Early Detection; Cancer in Men Rising; Diet Drives Colon Cancer
3.
Asymptomatic Brain Metastases in EGFR-Mutant NSCLC
4.
Mapping lifelong chronic health risks for childhood cancer survivors
5.
Adding Chemo to Osimertinib Doubles PFS in Advanced NSCLC
1.
Respiratory Ramifications of Systemic Disease: A Comprehensive Review
2.
Revolutionizing Lung Cancer Treatment: Exploring the Benefits of Wedge Resection Surgery
3.
Trends in Incidence, Care, and Surgery for Medullary Thyroid Cancer: A Review
4.
Cancer Care Advances: Metformin, Digital Tools, and Artificial Renal Support
5.
Molecular Mechanisms, Clinical Efficacy, and Stem Cell Therapy Integration in Leukemia Treatment
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Treatment Paradigm for Patients with R/R Adult B-cell ALL- Expert Discussions
2.
First Line Combination Therapy- The Overall Survival Data in NSCLC Patients
3.
Guideline Recommendations of Lorlatinib as First-Line Treatment for ALK+ NSCLC
4.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part II
5.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part III

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge