Cutaneous Melanoma: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Cutaneous melanoma is an aggressive skin malignancy with high potential for metastasis and morbidity if not detected early. Disease prognosis depends on tumor thickness, ulceration, mitotic rate, and timely surgical intervention. We report a case of a middle-aged female presenting with a rapidly enlarging pigmented lesion on the upper back. This case highlights clinical presentation, dermoscopic and histopathological diagnostic evaluation, surgical and adjuvant management, and follow-up outcomes. The report underscores the importance of early detection, accurate staging, appropriate surgical excision, sentinel lymph node assessment, and structured follow-up to optimize patient survival and reduce recurrence risk.
Introduction
Melanoma is a malignant tumor of melanocytes, accounting for a significant proportion of skin cancer-related mortality worldwide. Risk factors include fair skin, ultraviolet (UV) exposure, family history, and presence of multiple or atypical nevi. Early diagnosis is crucial, as prognosis worsens with increasing Breslow thickness, ulceration, or regional/distant metastasis. Standard management includes wide local excision, sentinel lymph node biopsy (SLNB), and consideration of adjuvant systemic therapy in high-risk cases. This report presents the clinical course, diagnostic challenges, management strategy, and outcome of a patient with cutaneous melanoma.
Case Report
Patient History
A 52-year-old female presented to the dermatology clinic with a 3-month history of a pigmented lesion on her upper back, which had rapidly increased in size and become irregular in color. The patient reported occasional bleeding and mild tenderness. She had a history of extensive sun exposure but no prior history of skin cancer or family history of melanoma. There was no history of systemic symptoms such as weight loss or fatigue.
Clinical Examination
On examination, a 2.5 cm × 2 cm asymmetrical, irregularly bordered, multicolored (black, brown, and blue) lesion was noted on the right upper back.

The lesion was elevated, firm, and showed areas of ulceration. No other suspicious cutaneous lesions were noted. Regional lymph nodes were not palpable. Full skin and systemic examination were otherwise unremarkable.
Clinical Evaluation
Differential Diagnosis
-
Malignant melanoma
- Dysplastic nevus
- Seborrheic keratosis
- Pigmented basal cell carcinoma
- Dermatofibroma
Investigations
Dermoscopic examination

revealed asymmetry, irregular pigmentation, atypical network, and blue-white veil suggestive of melanoma.

Excisional biopsy with 1–2 mm margins was performed. Histopathology confirmed invasive superficial spreading melanoma, Breslow thickness 2.2 mm, Clark level IV, mitotic rate 3/mm², and absence of lymphovascular invasion.
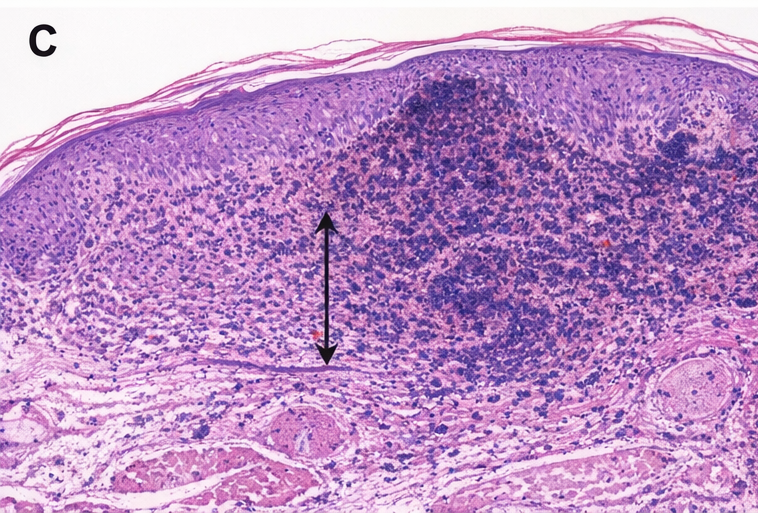
Immunohistochemistry was positive for S-100, HMB-45, and Melan-A. Ultrasound of regional lymph nodes showed no suspicious enlargement. Staging investigations including CT scan of the chest and abdomen showed no evidence of metastasis (Stage IB).
Management and Outcome
Management Strategy
The patient underwent wide local excision with 2 cm margins and sentinel lymph node biopsy, which was negative for metastatic involvement.

Postoperative recovery was uneventful. The patient was counseled on sun protection and skin self-examination. Multidisciplinary team discussion concluded that adjuvant systemic therapy was not indicated at this stage. Structured follow-up with dermatology and oncology was planned every 3 months for the first year.
Follow-Up and Outcome
At 12 months follow-up, the patient remained completely disease-free, with no evidence of local recurrence, regional lymph node involvement, or distant metastasis. The surgical site healed well, with an unremarkable scar, and dermoscopic surveillance revealed no new suspicious pigmented lesions. Routine clinical examinations, including full skin checks, and imaging assessments were performed regularly, reinforcing vigilance for early detection of any recurrence or secondary primary melanomas. The patient was counseled to continue monthly self-skin examinations, maintain strict sun protection measures, and promptly report any changes in existing or new lesions. Structured follow-up continues to be essential to ensure ongoing disease monitoring, reinforce preventive strategies, and provide early intervention if any abnormal findings arise. Overall, the patient’s condition remains stable, highlighting the effectiveness of timely surgical management, careful surveillance, and patient engagement in long-term melanoma care.Discussion
Melanoma prognosis is strongly influenced by early diagnosis, prompt intervention, and timely surgical management, as delayed recognition significantly increases the risk of metastasis and mortality. Key prognostic factors include Breslow thickness, the presence or absence of ulceration, mitotic index, and sentinel lymph node biopsy (SLNB) status, all of which guide staging, risk stratification, and treatment planning. Dermoscopy plays a critical role in early detection by allowing clinicians to identify subtle and characteristic features of melanoma, such as asymmetry, atypical pigment network, and irregular vascular patterns, which are often not visible to the naked eye. Wide local excision with appropriately determined margins remains the cornerstone of surgical management, ensuring complete tumor removal while minimizing local recurrence. SLNB is particularly indicated for intermediate-thickness tumors, providing valuable prognostic information and guiding decisions about adjuvant therapy. For patients with high-risk features or positive nodal involvement, adjuvant treatment options—including immunotherapy with checkpoint inhibitors or targeted therapy for tumors with actionable mutations—can significantly improve disease-free survival. Regular, structured follow-up is essential for the early detection of recurrence, regional nodal involvement, or the development of new primary melanomas, and should include clinical examination, imaging as indicated, and patient education on self-monitoring. By combining early diagnosis, meticulous surgical intervention, evidence-based adjuvant therapy, and vigilant follow-up, clinicians can substantially improve outcomes and long-term survival for patients with melanoma.
Conclusion
Cutaneous melanoma is a potentially life-threatening malignancy that requires prompt recognition, accurate histopathological evaluation, and timely surgical management to optimize patient outcomes. Early diagnosis is critical, as prognosis significantly worsens with increasing tumor thickness, ulceration, or regional metastasis. Comprehensive care involves not only surgical excision but also sentinel lymph node assessment, consideration of adjuvant therapy when indicated, and structured, long-term follow-up to monitor for recurrence or new primary lesions. Patient education plays a central role, including guidance on self-skin examination, recognition of suspicious lesions, strict UV protection, and awareness of risk factors. Multidisciplinary coordination among dermatologists, oncologists, and surgeons is essential to ensure evidence-based decision-making, timely interventions, and continuity of care. Prevention strategies, early detection, and vigilant monitoring collectively improve survival rates and quality of life for patients with melanoma.
References
- Gershenwald JE, Scolyer RA, Hess KR, et al. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin. 2017;67(6):472–492.
- Whiteman DC, Green AC, Olsen CM. The growing burden of invasive melanoma: projections of incidence rates and numbers of new cases in six susceptible populations through 2031. J Invest Dermatol. 2016;136(6):1161–1171.
- Leiter U, Keim U, Garbe C. Epidemiology of melanoma and nonmelanoma skin cancer—characteristics, differences, and trends. Dermatol Pract Concept. 2014;4(3):7–14.
- Morton DL, Thompson JF, Cochran AJ, et al. Sentinel-node biopsy or nodal observation in melanoma. N Engl J Med. 2006;355:1307–1317.
- Swetter SM, Tsao H, Bichakjian CK, et al. Guidelines of care for the management of primary cutaneous melanoma. J Am Acad Dermatol. 2019;80(1):208–250.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Breast Cancer Patients Living Longer Post-Medicaid Expansion
2.
Error on the MGUS-Autoimmune Disease Association.
3.
Patients with chronic myeloid leukemia who take nilotinib are at higher risk for diabetes and hyperlipidemia.
4.
The majority of cancer medications that receive expedited approval end up failing confirmatory trials.
5.
Unified Neuro/Psych Residency Program: New Proposal.
1.
Optimizing Melanoma Treatment: Strategies in Diagnosis, Clinical Research, and Physician Training
2.
Hemoglobin C: Understanding its Role in Sickle Cell Disease
3.
Beyond the Human Eye: How AI Is Redefining Brain Cancer Diagnosis Through Advanced Imaging
4.
Understanding Abemaciclib: A Breakthrough Treatment for Breast Cancer
5.
The Growing Challenge of Haematological Malignancies in Older Adults
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Revolutionizing Treatment of ALK Rearranged NSCLC with Lorlatinib - Part II
2.
Exploring Potentials of Lorlatinib: The Third Generation ALK-TKI Through CROWN Trial
3.
Molecular Contrast: EGFR Axon 19 vs. Exon 21 Mutations - Part VII
4.
A Conclusive Discussion on CROWN Trial and the Dawn of a New Era in Frontline Management of ALK+ NSCLC
5.
Efficient Management of First line ALK-rearranged NSCLC - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge