Becker Nevus: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Becker nevus is a benign cutaneous hamartoma characterized by hyperpigmentation and often associated with hypertrichosis. It typically presents during adolescence and shows a strong male predominance. Although primarily a cosmetic concern, it may occasionally be associated with underlying developmental anomalies, constituting Becker nevus syndrome.
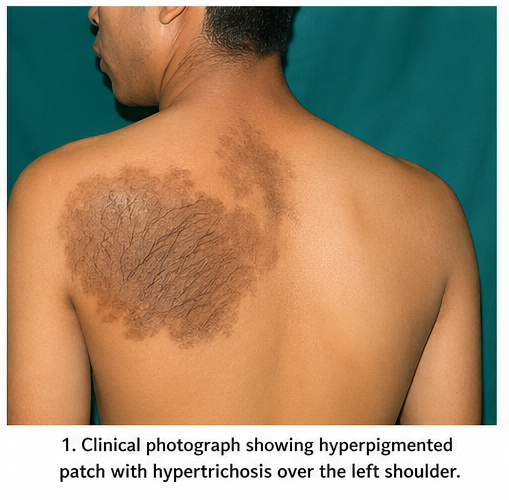
We report the case of a 19-year-old male who presented with a gradually enlarging hyperpigmented patch over the left shoulder associated with increased hair growth. Clinical and dermoscopic evaluation confirmed the diagnosis of Becker nevus. The patient was managed conservatively with counseling and offered laser therapy for cosmetic improvement, resulting in satisfactory outcomes.
This case underscores the importance of accurate clinical diagnosis, differentiation from other pigmented lesions, and individualized management strategies in patients with Becker nevus.
Introduction
Becker nevus, also referred to as Becker melanosis, is a cutaneous hamartoma involving epidermal and adnexal structures. First described in 1949, it typically manifests as a unilateral, irregularly bordered hyperpigmented patch, most commonly located on the upper trunk, shoulder, or chest.
The lesion often becomes apparent during adolescence, coinciding with hormonal changes, and may progressively darken and develop hypertrichosis. The condition is thought to be androgen-dependent, which explains its higher prevalence in males and the presence of terminal hair growth within the lesion.
Although Becker nevus is benign, its clinical significance lies in its potential association with musculoskeletal or developmental abnormalities in rare cases, termed Becker nevus syndrome.
Risk factors and associations include:
• Male gender predominance
• Onset during puberty
• Hormonal influence (androgen sensitivity)
• Rare association with skeletal or breast hypoplasia
Clinically, patients often present with cosmetic concerns due to pigmentation and hair growth rather than functional impairment.
Case Report
Patient History
A 19-year-old male presented to the dermatology outpatient department with complaints of:
• A dark patch over the left shoulder
• Gradual increase in size over 3 years
• Excessive hair growth over the lesion
• No associated itching, pain, or discharge
The lesion was first noticed at the age of 16 and had progressively increased in pigmentation and hair density. There was no history of trauma, drug intake, or preceding inflammation in the affected area.
The patient had no significant past medical history and no family history of similar lesions or dermatological conditions.
Clinical Examination
General Examination
• Patient was well-built and well-nourished
• Vital signs were stable
• No systemic abnormalities detected
Dermatological Examination
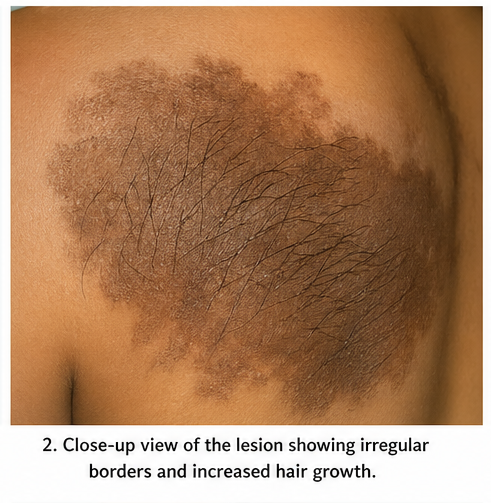
• A single, well-defined but irregularly bordered hyperpigmented patch measuring approximately 12 × 8 cm over the left shoulder
• Color varied from light brown to dark brown
• Presence of coarse terminal hair over the lesion (hypertrichosis)
• Surface was smooth, with no scaling or nodularity
• No signs of inflammation or ulceration
There were no similar lesions elsewhere on the body.
Systemic Examination
• No evidence of musculoskeletal deformities
• No breast asymmetry or hypoplasia
• Neurological examination was normal
Clinical Evaluation
Differential Diagnosis
Based on clinical presentation, the following conditions were considered:
• Becker nevus
• Congenital melanocytic nevus
• Café-au-lait macule
• Post-inflammatory hyperpigmentation
• Nevus spilus
The presence of late onset, hypertrichosis, and progressive pigmentation strongly suggested Becker nevus.
Investigations
Dermoscopy
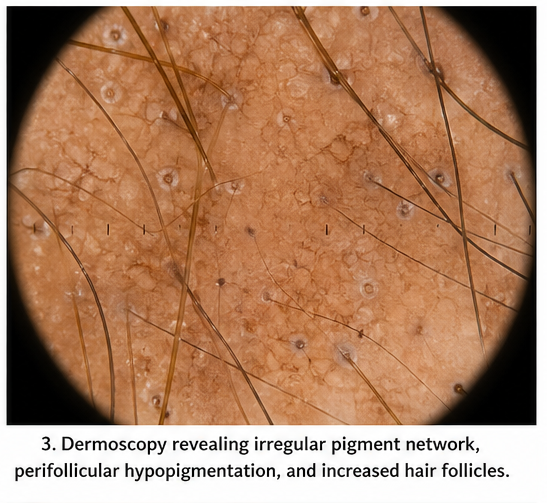
Dermoscopy revealed:
• Irregular pigment network
• Perifollicular hypopigmentation
• Increased hair follicles
• No atypical vascular structures
These findings were consistent with Becker nevus.
Histopathology (Optional, not performed in this case)
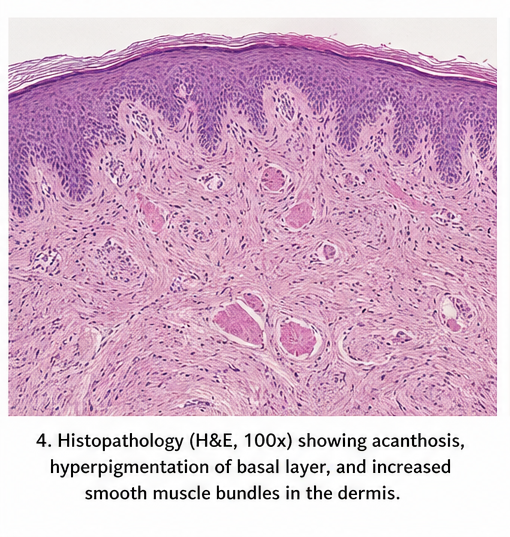
Although not required due to classical presentation, histopathological features typically include:
• Acanthosis and hyperkeratosis
• Increased basal layer pigmentation
• Smooth muscle hyperplasia in the dermis
• Increased melanocyte activity
Laboratory Investigations
• Routine blood investigations were within normal limits
No imaging was required as there were no associated systemic abnormalities.
Diagnosis
Based on clinical and dermoscopic findings, a diagnosis of Becker nevus involving the left shoulder was established.
Management and Outcome
Management Strategy
The treatment approach was guided by:
• Cosmetic concerns
• Extent of pigmentation
• Presence of hypertrichosis
• Patient preference
Since Becker nevus is a benign condition, management focused primarily on cosmetic improvement and patient reassurance.
Treatment Options Discussed
Conservative Management
• Patient education regarding benign nature of the condition
• Reassurance to alleviate anxiety
• Regular follow-up to monitor any changes
Medical Therapy
Topical therapies have limited effectiveness but may include:
• Topical anti-androgens (in selected cases)
• Pigment-reducing agents (variable response)
Laser Therapy
The patient was counseled regarding laser-based interventions:
• Q-switched lasers for pigmentation reduction
• Long-pulsed lasers for hair removal
Laser therapy offers moderate improvement but may require multiple sessions and has variable outcomes.
Intervention and Follow-Up
The patient opted for conservative management initially, with consideration for future laser therapy.
At 3-Month Follow-Up:
• No progression in lesion size
• Patient reassured and satisfied with counseling
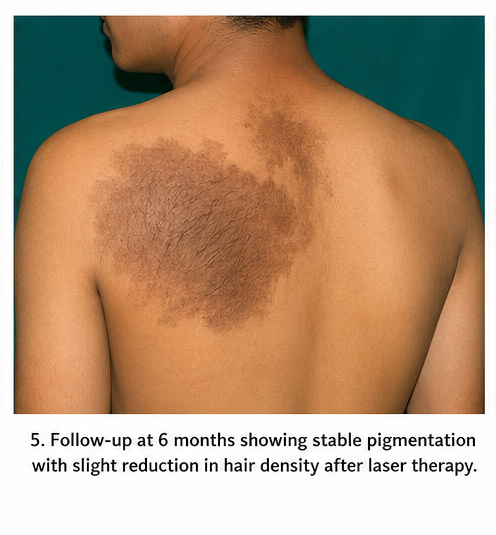
At 6-Month Follow-Up:
• Lesion remained stable
• Patient opted for trial of laser hair reduction
At 9-Month Follow-Up:
• Mild reduction in hair density
• Slight improvement in pigmentation
• No complications observed
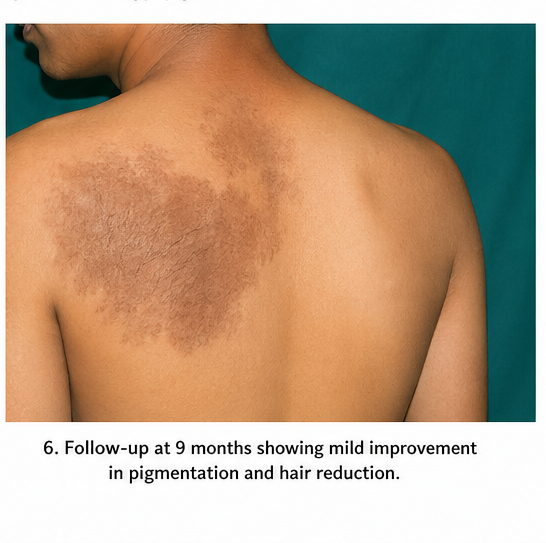
Overall, the patient reported improved cosmetic satisfaction.
Discussion
Pathophysiology
Becker nevus is considered a cutaneous hamartoma involving:
• Epidermal melanocytes
• Hair follicles
• Smooth muscle components
The exact etiology remains unclear, but androgen receptor hypersensitivity is believed to play a key role. Increased androgen activity explains:
• Onset during puberty
• Male predominance
• Associated hypertrichosis
Epidemiology
• More common in males (male-to-female ratio approximately 5:1)
• Typically appears during adolescence
• Most commonly affects the upper trunk and shoulders
Becker Nevus Syndrome
In rare cases, Becker nevus may be associated with:
• Ipsilateral breast hypoplasia
• Skeletal abnormalities
• Muscular defects
This constellation is termed Becker nevus syndrome and requires thorough evaluation.
Diagnostic Considerations
Diagnosis is primarily clinical. Key distinguishing features include:
• Late onset (adolescence)
• Hyperpigmentation with irregular borders
• Hypertrichosis
• Unilateral distribution
Dermoscopy aids in confirmation, while biopsy is reserved for atypical cases.
Treatment Considerations
There is no definitive cure for Becker nevus. Management focuses on cosmetic improvement.
Pigmentation Treatment:
• Q-switched Nd:YAG laser
• Fractional lasers
Hair Removal:
• Laser hair reduction (diode or alexandrite lasers)
Limitations:
• Variable response
• Risk of recurrence
• Multiple sessions required
Complications
Becker nevus itself is benign and not associated with malignant transformation. However, potential concerns include:
• Cosmetic disfigurement
• Psychological impact
• Rare association with syndromic features
Laser therapy complications may include:
• Post-inflammatory hyperpigmentation
• Hypopigmentation
• Skin irritation
Prognosis
The prognosis of Becker nevus is excellent.
Key factors influencing outcomes:
• Extent of lesion
• Patient expectations
• Response to cosmetic treatments
The lesion typically stabilizes after adolescence and does not progress significantly thereafter.
Conclusion
Becker nevus is a benign dermatological condition characterized by hyperpigmentation and hypertrichosis, most commonly presenting during adolescence. Although it poses no medical risk, it can have significant cosmetic and psychological implications.
This case highlights the importance of recognizing classical clinical features to avoid unnecessary investigations and interventions. Dermoscopy serves as a useful non-invasive diagnostic tool, while biopsy is rarely required.
Management should be individualized, focusing on patient education, reassurance, and cosmetic improvement when desired. Laser therapies offer promising results, although outcomes may vary.
Early identification and appropriate counseling play a crucial role in improving patient satisfaction and quality of life. Increased awareness among clinicians can facilitate accurate diagnosis and prevent mismanagement of this benign condition.
References
- Becker, S. W. (1949). Concurrent melanosis and hypertrichosis in distribution of nevus unius lateris. Archives of Dermatology and Syphilology. https://pubmed.ncbi.nlm.nih.gov/18116269/
- Happle, R. (1997). Becker nevus syndrome. Journal of the American Academy of Dermatology. https://pubmed.ncbi.nlm.nih.gov/9039171/
- Kim, Y. J., et al. (2008). Clinical and histopathological characteristics of Becker's nevus. Journal of Dermatology. https://pubmed.ncbi.nlm.nih.gov/18789063/
- Patrizi, A., et al. (2012). Becker nevus: Clinical features and treatment options. Pediatric Dermatology. https://pubmed.ncbi.nlm.nih.gov/22384933/
- Sardana, K., et al. (2014). Lasers for Becker’s nevus: A systematic review. Journal of Cutaneous and Aesthetic Surgery. https://pubmed.ncbi.nlm.nih.gov/25284856/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge